Foster Parent Handbook
Chapter 6
Colour Code Key:
Fosterplus Policies, Procedures and Guidance
Legislation and Government Guidance
General Sources and Good Practice Information
The Child’s Wishes and Feelings
Expressing your views
“My views will always be sought and my choices respected, including when I have reduced capacity to fully make my own decisions.”
“If I am unable to make my own decisions at any time, the views of those who know my wishes, such as my foster parent, independent advocate, formal or informal representative, are sought and taken into account.”
Health and Social Care Standards: 2.11 and 2.12
Children’s Guides
Every fostering service must produce a written Children’s Guide, which includes:
- A summary of what the fostering service sets out to do for children
- How they can find out their rights
- How to contact Care Inspectorate, if they wish to raise a concern with inspectors
- How to secure access to an independent advocate
The supervising social worker ensures that every child (subject to age and understanding) receives an age appropriate copy of our Children’s Guide, at the point of placement. It is the responsibility of foster parents to go through this with children and young people and to explain the contents. Where a child requires it, we will make the guide available in translation or through suitable alternative methods of communication, such as pictures, tape recording etc. If foster parents think this is required, they should discuss it with their supervising social worker.
Participation of Children and Young People
Listening to children and young people – what is the role of foster parents?
Fosterplus has since its inception had a commitment to participation at all levels of the organisation including, involving stakeholders in shaping the development of the service provided. We will talk and listen to the users of our services and make changes where possible in light of what we learn.
Fosterplus Participation Strategy – can be downloaded from CHARMS/Download
It is essential that children and young people are empowered to communicate their views on all aspects of their care and support. Within a foster home, children should receive personalised care and be allowed to exercise reasonable choice and independence in the food they eat and are able to prepare, clothes and personal requisites they buy etc. This should happen within reasonable limits set by each foster family.
Foster parents can play an important role in helping children and young people to take up issues with Fosterplus or their local authority, and can also help children understand how their views have been taken into account or to understand why their wishes or concerns have not been acted upon.
Fosterplus young people’s participation groups
Each local Fosterplus office runs a range of structured activities for young people of different ages, usually during school holidays. There are also participation groups where young people can meet together to share experiences and contribute their ideas to the running of Fosterplus. Your local office will keep you informed of events being organised.
Independent Advocacy Services
“I am supported to use independent advocacy if I want or need this.”
Health and Social Care Standards: 2.4
Why might a child need an advocate?
Foster parents are often the best champions for the children they care for and you should certainly see your role as that of a ‘pushy parent’ when it comes to dealing with services such as Education and Health; but sometimes you may not be in the best position to advocate for a young person. For example, a child or young person may wish to express dissatisfaction with their foster parent or their social worker and, in some situations, foster parents will feel unable to represent the child’s wishes and views as they may conflict with their own.
Children also may feel that they are not being listened to and that adults are making major decisions about their lives without treating their views seriously. They may not feel confident enough to challenge adults on their own, or may not know the right way to make sure their views are heard and acted upon.
What does an independent advocate do?
The role of an independent advocate is to support young people in making sure their views are properly represented, either by enabling the young person to speak for themselves or speaking on their behalf. All local authorities are required to provide independent advocacy schemes to which foster children must have access. It is very important that foster parents ensure that the children in their care are aware of their right to advocacy services and actively encourage them to use such services.
How does a child or young person access an advocate?
The welcome pack given to all young people when they come into the care of Fosterplus contains information regarding advocacy services such as the Children’s Rights Officer and Who Cares? Scotland; there is also information on how to give feedback about the service; It is important to bring this to their attention. Their local authority social worker should also be ensuring they have the information they need.
Children and Young People’s Commissioner
The role of the Children’s Commissioner in Scotland has a duty to promote and protect the rights of all children in Scotland in accordance with the United Nations Convention on the Rights of the Child.
Children and young people from all over the Scotland helped choose Bruce Adamson as their current Commissioner. They interviewed him about how he would help young people know more about their rights and found out his plans for the job by asking him lots of questions.
It is his job to make life better for all children and young people by making sure their rights are respected and realised and that their views are taken seriously.
He and his team looks after the rights of
- Everyone in Scotland under 18
- Everyone in Scotland under 21 who has been looked after or in care
There are various ways of making contact with the Commissioner either on line, by phone or text. There is also a link on their website with HAPPY TO TRANSLATE which is a unique and innovative national scheme which bridges communication gaps between organisations and service users who struggle to communicate in English.
Children & Young People’s Commissioner Scotland
Children and Young People’s Commissioner Scotland
Bridgeside House
99 McDonald Road
Edinburgh EH7 4NS
Tel: 0131 346 5350
Contact can be made by an online email service at
Web: https://www.cypcs.org.uk/contact/
Young People’s Freephone: 0800 019 1179
Or by Text 0770 233 5720 Texts will be charged at your standard network rate
In addition, there is the national CHILDLINE help line who can be contacted confidentially on 0800 1111 – the service is free and fully confidential and young people can contact them anonymously if they wish for information, advice or guidance.
Child’s Identity
Promoting a positive identity and valuing diversity
Identity and Heritage
“I am supported to be emotionally resilient, have a strong sense of my own identity and wellbeing, and address any experiences of trauma or neglect.”
Health and Social Care Standards: 1.29
Many looked after children have low self-worth and a very poor sense of their own identity. Many come from families that are subject to multiple problems and marginalisation. The Human Rights Act 1998, the Equalities Act 2010, the UN Convention on the Rights of the Child, as well as the Children (Scotland) Act 1995 all require that every individual child who is looked after should be cared for in a way that respects, recognises, supports and celebrates their identity and provides them all with care, support and opportunities to maximise their individual potential.
UN Convention on the Rights of the Child
The UN Convention on the Rights of the Child can be downloaded via the UNICEF website at: http://www.unicef.org/crc/
Equal opportunities
Fosterplus is committed to a positive policy of equal opportunities in the delivery of its services to children and foster parents, employment of staff and recruitment of foster parents. We will actively oppose all forms of discrimination carried out on the grounds of age, disability, gender reassignment, marriage and civil partnership, pregnancy and maternity, race, religion or belief, sex, and sexual orientation.
All foster parents and staff will receive training on equality and diversity practice and expectations.
Trans-racial and trans-cultural placements
Fosterplus believes that a child’s racial and cultural background is fundamental to their identity and needs to be maintained and encouraged. Foster parents have a key role to play in enabling young people to feel secure in their sense of identity. This will often be best achieved through placements into families with same or similar racial and cultural backgrounds.
Where such placements are not available, it may still be in the child’s better interests to place them with a family from a different racial or cultural background. We recognise that an important principle in working with children from different cultures is to acknowledge that this requires special commitment, knowledge and skills, which need to be developed if young people of differing ethnic and cultural backgrounds are to grow up with a positive image of themselves.
Fosterplus will offer training, support, information and guidance for foster parents and social work staff to enable them to meet the needs of each child, and to maintain a commitment to equal opportunities. Foster parents are expected to undertake the mandatory training course Equality and Diversity within their first year of approval by the agency.
We also record and monitor the ethnicity, religion and spoken languages of children referred to us and placed with our foster families, as well as those who enquire about fostering with us. This data is used to inform the continuing development of services that meet the cultural and racial needs of foster children.
Promoting cultural identity
The practical ideas that follow have four important aims:
- To promote the child’s cultural identity.
- To give the child positive images of their identity.
- To prepare the child for the society in which they will be growing up.
- To learn about and share in the child’s culture.
The following is a list of some of the ways in which foster parents and social workers can actively involve themselves in any foster child’s culture, whether or not they share the same culture with them. The list is by no means definitive and each idea does not apply to all cultures, but it does include some important suggestions:
- Find out about special dietary rules.
- Find out about essential cultural customs, like hair and skin care.
- Make sure you have a stock of appropriate toys, books, etc.
- Find out about the rules of religious observance.
- Involve the foster family and the child with other families who reflect the child’s heritage.
- Encourage the child to keep contact with members of their original community, (the foster parents and their family should also meet them, where this is appropriate).
- Learn about the historical foundations of the child’s culture and share these with the child.
- Make contact with the local black or other minority ethnic community and attend social events with the child.
- Be aware of racism in the language you use and examine your attitudes to it. Help the child find ways of coping with it.
- Encourage the reading of black literature and the watching of television programmes directed towards ethnic minorities.
- Encourage mother-tongue speaking and learning.
Foster parents must respect parents’ wishes and encourage all children to value their background. Foster parents should aim to care for the child in accordance with the parents’ views. Birth parents may be greatly distressed if their child breaks food laws or the observances of religion.
Making these efforts will show children in care that their foster parent and their social worker value their culture, and that any differences between them are manageable. The efforts will be rewarded by a much more real understanding of the child in your care. Foster parents can probably think of many ways in which they can involve themselves in a child or young person’s culture. On the other hand, if the culture is very unfamiliar to them it may feel daunting, and if foster parents are not sure about how to go about seeking advice and making contact with their local black African, Asian, or other minority ethnic community, they should expect help, advice and support from the child’s social worker, and their supervising social worker.
Religion
We expect foster parents to care for a child’s spiritual and moral well-being as well as their physical and emotional development. Foster parents must not impose their own religious beliefs upon children and young people, even where the child may not declare themselves to be of any particular faith; but making them familiar with different beliefs may help them to develop their own ideas as they get older.
Information about a child’s religious beliefs should be provided by the child, his/her parents and/or social worker at the beginning of a placement and detailed in the placement plan, so that there is a clear understanding of expectations with respect of religion. This includes the religious background of a child’s family, the rules of religious observance, and the expectations regarding attendance at a place of worship.
Foster parents may need to take a child to and collect them from a place of worship, and must be prepared to do this. Foster parents should actively familiarise themselves with the values and practices of the child’s religious faith so that, for example, important dates in the child or young person’s religious calendar can be observed.
Dealing with discrimination
Children and young people may respond to prejudicial attitudes and discrimination by feeling ashamed, angry, rejected, and it may lower their sense of self-worth. For them to feel comfortable, foster parents and social workers need to feel comfortable too. Foster parents and social workers should help the child or young person to understand the nature of prejudice and prepare them to meet it and support them when they have to cope with it. It is a shared duty to take positive action to combat discrimination on the grounds of culture, religion, ethnicity or language.
Birth certificates
If a birth has been registered then a birth certificate is available recording the details of the child’s birth. If a copy of a child’s birth certificate is required, foster parents should contact the child’s social worker or seek advice from your supervising social worker.
Passports
Many foster children do not have a passport at the point they are first looked after. It is important that the potential for holidays and other trips abroad (e.g. school trips) is covered in the placement plan and that there is clarity about how a passport is to be obtained. This will be the responsibility of the child’s social worker and the United Kingdom Passport Agency provides guidance for social workers seeking to obtain a passport for a looked after child.
Where there are already plans in place for a holiday or other trip and the child does not have a passport, it is best to formally request that a passport be obtained as a matter of urgency. The written request should go to the supervising social worker to be passed on to the responsible authority, and should include:
- The reason for the request.
- The wishes of the child.
- The views of the parent/s, if known.
- The views of the foster parent/s.
The child’s social worker should obtain and complete the necessary application for the child or assist the child to complete the necessary application form.
If the child/young person is accommodated, their parents must be consulted with a view to obtaining their agreement. In such instances, good practice would suggest that involving the parent in the passport application process is recommended. Should the parent/s refuse to give consent and this is deemed unreasonable, then the child’s social worker may have to take advice from their Legal Services.
Life story work
What is life story work?
Children who live with their birth families generally have plenty of opportunity to know and learn about the events in their lives. These children generally grow up surrounded by their family members and they accept and feel secure about their place in the family. Their knowledge of who they are is built up from personal memories – good and bad – photographs, anecdotes and family folklore. All this is the foundation on which people build their self-image and become a secure adult.
All children are entitled to accurate information about their past and their family, but children separated from their birth families are often denied this opportunity. Many children come to blame themselves for being separated from their families and believe they are unlovable. Some children, particularly young children, can seem to live in the present and to forget the past. If a child has had a particularly unhappy time, foster parents and local authority social workers may also be tempted to try to protect them by encouraging them to forget the past. Though some memories will fade in the long term, curiosity – the deep need to know about their parents and understand their history in search of their true identity – will almost certainly surface, particularly when children are in their teens.
Compiling facts about their lives, and the significant incidents and the people in them, helps children to begin to understand and accept their past and move forward into the future. Life Story Work is a way of identifying and capturing the child’s past both by collating material such as photos, videos, mementos and written records, but also writing down people’s recollections of the child. Such information can be kept in a Life Story Book and Memory Box. The child’s social worker usually undertakes the sensitive task of compiling a life story book with the child, often in collaboration with the foster parent who has an important role in gathering material for the book.
The other important task for foster parents is to talk with the child in a way they can understand, about the fact they are not living at home and the reasons for this. It will be important for the foster parents to give them words to help explain their present circumstances and to allow them to accept those circumstances.
In summary, life story work can help the child feel comfortable with their past and reinforce their sense of identity and worth.
Ways to gather information for life story work
Written information – keeping regular records about the child’s development: when they walked and talked; what toys they liked; what food they liked etc. When deciding on what information to store in trust for the child, it is a good idea to think about the sorts of things your own children asked you about when they were younger. Also record factual information, such as full address of the playgroup or school attended.
Photographs and/or videos – taking these on a regular basis and on special occasions. It is important that, however brief, you take pictures of the child’s time in your family. Photographs of the foster parents and their family, foster home, child’s school and friends, pets, and of the child’s parents and family, may all be very important in the future. Take photographs of favourite activities, significant incidents, holidays, birthdays, weddings, parties and religious festivals. Write the date, location and names of people in the photo on the back. NB: Polaroid and computer generated photos fade. Use regular film and/or retain photos in digital format.
If children are reluctant to have their picture taken, then please respect this. Usually, with time and the excitement of an event, this self-consciousness passes. It is always possible that children may be reticent to have photographs taken because this was part of their previous abuse by an adult.
Mementos – keeping mementos of places visited, holidays shared, some playgroup pictures, school reports and so on. Retain certificates from school, sporting or educational awards, and anything else you or the child feel is important. These offer tangible evidence that the child had many experiences and provide a record of them.
Records of family time with birth families – keeping information about their family: from what they look like to what they were good and bad at. This is especially important if the child is not returning home, because it may eventually help them understand why this was not possible.
What happens to the life story book?
The life story book and other information in a memory box belongs to the child and should go with them when they leave a foster home. At the point a child or young person is moving on, you should discuss with the supervising social worker the best way to pass on information held in a memory box and/or life story book.
Children’s Behaviour and Relationships
Self-Regulation and Behaviour Management Training
In addition to the Secure Base Model, Fosterplus has also introduced a positive behaviour support training programme called Self-Regulation and Behaviour Management:
- Support foster parents and other involved professionals in developing knowledge and skills in positively responding to challenging behaviour.
- Promote the on-going development of resilience, de-escalation skills and confidence in children, young people and their foster parents.
The importance of secure base
The Secure Base Model provides a positive integrated framework that underpins Fosterplus’s practice, service delivery and learning. We have been running Introduction to The Secure Base Model programmes for both foster parents and support staff since 2016. This has included the senior leadership team, all managers, social workers and administrators, reflecting a shared vision and ambition to embed the secure base model throughout the organisation at every level. This is about building on and developing the foundations from which we all support, understand, share experience and improve the ordinary life experiences and chances of the children and young people who live within our service.
A secure base is at the heart of any successful caregiving environment – whether within the birth family, in foster care, residential care or adoption. A secure base is provided through a relationship with one or more caregivers who offer a reliable base from which to explore and a safe haven for reassurance when there are difficulties. Thus a secure base promotes security, confidence, competence and resilience.
Understanding children’s behaviour
Many children who are fostered have had experiences that give them little reason to trust adults. They have developed behaviours based on a need to try to protect themselves and to control their relationships and environments. Attachment theory suggests that exposure to warm, consistent and reliable caregiving can change children’s previous expectations, both of close adults and of themselves. The role of adults who can provide secure base caregiving, therefore, is of central importance.
The Secure Base Model provides a positive framework for therapeutic caregiving, which helps infants, children and young people to move towards greater security and builds resilience. It focuses on the interactions that occur between caregivers and children on a day to day, minute by minute basis in the home environment. But it also considers how those relationships can enable the child to develop competence in the outside world of school, peer group and community.
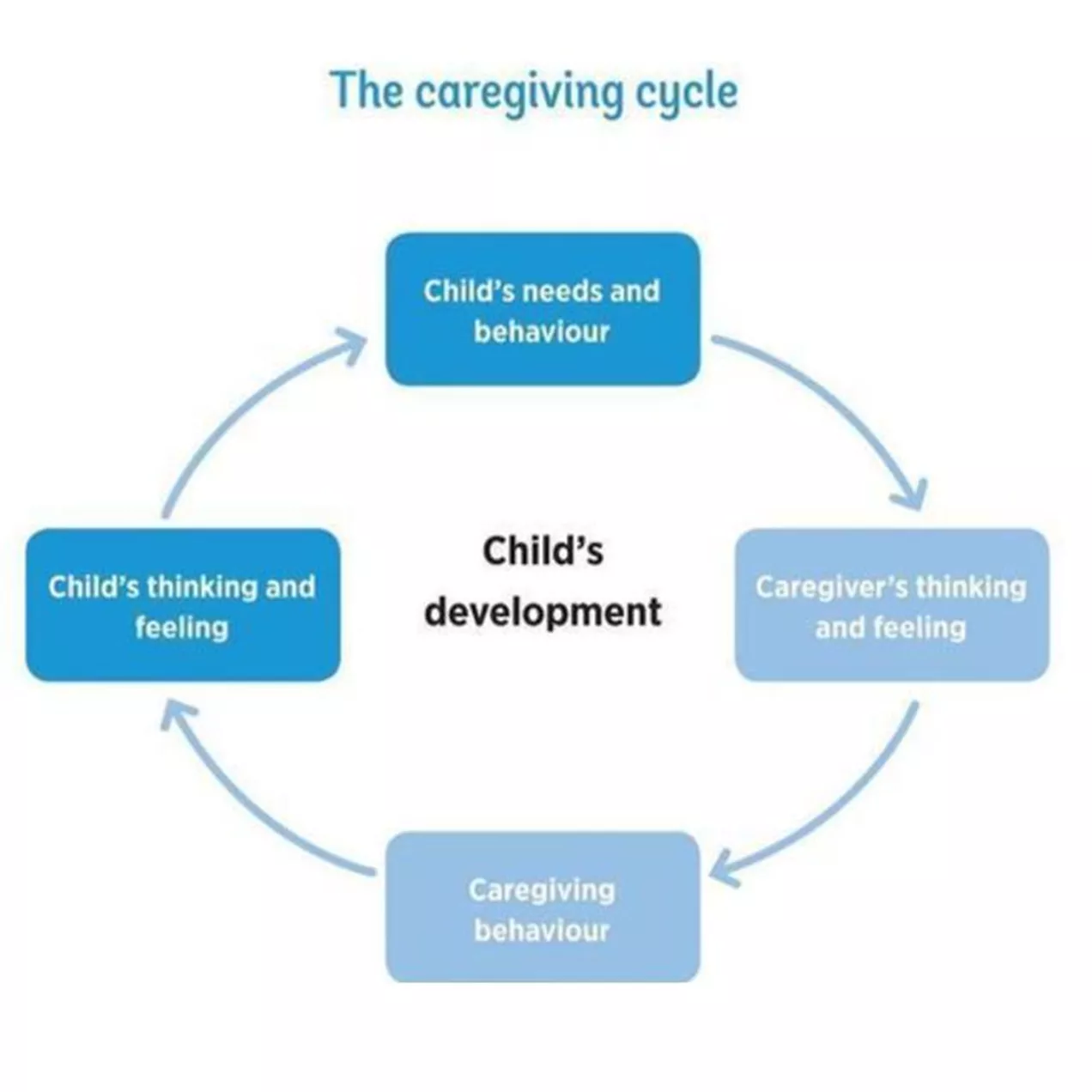
It can be helpful, first, to think about caregiver/child interactions as having the potential to shape the thinking and feeling and ultimately the behaviour of the child.
This cycle begins with the child’s needs and behaviour and then focuses on what is going on in the mind of the caregiver. How a caregiver thinks and feels about a child’s needs and behaviour will determine his or her caregiving behaviours. The caregiver may draw on their own ideas about what children need or what makes a good parent from their own experiences or from what they have learned from training. The caregiving behaviours that result convey certain messages to the child. The child’s thinking and feeling about themselves and other people will be affected by these messages and there will be a consequent impact on his or her development. This process is represented in a circular model, the caregiving cycle, which shows the inter-connectedness of caregiver/child relationships, minds and behaviour, as well as their ongoing movement and change.
Information and support to foster parents around behaviour
Foster parents must be given all the relevant information about the child or young person placed with them to help them to provide a secure base, build positive relationships and manage behaviour. This must include information about previous challenging behaviour and advice about how this might be handled in the future. If this is not provided by the child’s social worker, the supervising social worker will follow this up.
The child’s placement plan must set out any specific behavioural issues that need to be addressed or approaches to be used.
Research tells us that it is of great importance for foster parents to realise and build on whatever strengths and abilities (‘resilience’) a child has. The Secure Base Model emphasises the critical role the foster parent (‘caregiver’) can have in creating the best possible environment for a child to build on and develop their resilience, by thoughtfully offering:
- Availability – Helping the child to trust
- Sensitivity – Helping the child to manage feelings and behaviour
- Acceptance – Building the child’s self-esteem
- Co-operation – Helping the child to feel effective and to be co-operative
- Family membership – Helping the child to belong
Availability – Approaches for helping children to build trust
N.B. It is important to choose only activities that the child is likely to accept and enjoy.
- Day-to-day activities
- Establish predictable routines around mealtimes, getting up and going to bed.
- Ensure that the child always knows where to find you when you are apart.
- Manage separations carefully, with open communication about why it is happening, how long it will be and clear ‘goodbyes’ and ‘hellos’.
- Use calendar or diary chart to help the child predict and anticipate events.
- Ensure that the child feels specially cared for and nurtured when ill, hurt or sad.
- Be ‘unobtrusively available’ if the child is anxious but finds it hard to talk or accept comfort (for example, suggest a ride in the car).
- Offer verbal and non-verbal support for safe exploration.
- Building trust when caregiver and child are apart.
- Allow child to take small item or photo from home to school.
- Use mobile phone or text to help child know that you are thinking of them.
- Place small surprise on child’s bed when he is at school to show you have thought about them during the day.
- Keep a ‘goodies tub’ in the kitchen and put small treats in it for child to have in the evening.
- Activities that help children to think about trusting.
- Ask child to draw a fortress or make one in clay or sand. Child may choose miniature toys or animals to stand for the main people in his life. Ask child to show and talk about which ones he would let into his fort and which ones he would keep out and why (from Sunderland 2000).
- Ask child to draw a bridge with themselves on one side and someone they trust on the other. Ask them to draw a speech bubble coming out of their mouth and write in it what they are thinking or saying. Do the same with the other person (from Sunderland 2000).
Games and activities that help to build trust:
- Hand holding games such as ‘ring a roses’.
- Clapping games.
- Reading stories with child on lap or sitting close.
- Leading each other blindfold.
- Face painting.
- 3-legged race.
- Throwing a ball or beanbag to each other.
- Bat and ball.
- Blowing and chasing bubbles together.
- Rocking, singing, gently holding child.
- Rub lotion onto each other’s hands and arms.
- Brush and plait hair, paint nails.
- Teaching a new skill or learning one together.
(Source: Providing a Secure Base, Gillian Schofield and Mary Beek, University of East Anglia, Norwich, UK)
Sensitivity – approaches for helping children to manage feelings and behaviour
N.B. It is important to choose only activities that the child is likely to accept and enjoy.
- Observe child carefully – perhaps keep a diary, note patterns, the unexpected etc. Try to stand in the child’s shoes.
- Anticipate what will cause confusion and distress for the child and avoid if possible.
- Read cues for support and comfort – be aware of ‘miscuing’.
- Express interest, at a level that is comfortable for the child, in his/her thoughts and feelings.
- Provide shared, pleasurable activity and a ‘commentary’ on the feelings experienced by self and child.
- Find time for interactions that promote synchrony of action, experiences, expressions of feeling (simple action rhymes and songs, clapping games for younger children, ball and beanbag games, learning a dance together, building or making something together, share an ‘adventure’ or new experience together, a game that involves a shared experience of both winning and losing).
- Make a ‘me calendar’ to help a child to see and remember what is going to happen next.
- Collect tickets, pictures, leaflets, stickers etc. and make an ‘experiences book’ to help a child to remember and reflect on positive events.
- Name and discuss feelings in everyday situations (happy, proud, sad, confused, angry, worried, peaceful, excited, guilty, lonely, pleased, etc. Also discuss mixed feelings and feelings that change over time.
- Play ‘sensory’ games (involving touch, sound, smell, observation).
- Use clay, paint, crayons to express feelings.
- Use play and real examples to make sense of the world, how things work, cause and effect.
- Encourage children to stop and think before reacting.
- Help children recover/repair the situation/make things better after losing control of feelings – praise them for doing this.
- Use stories or puppets to develop empathy in the child – ‘poor owl, how does he feel now his tree has been cut down’, etc.
- Use television programmes/films to focus on why people feel different things and how they can feel different things at the same time.
- Speculate on and give names to the possible feelings of others in everyday conversations.
(Source: Providing a Secure Base, Gillian Schofield and Mary Beek, University of East Anglia, Norwich, UK)
Acceptance – approaches for building self esteem
N.B. It is important to choose only activities that the child is likely to accept and enjoy.
- Praise child for achieving small tasks and responsibilities.
- Provide toys and games that create a sense of achievement.
- Liaise closely with nursery and school to ensure a sense of achievement.
- Use positive language. For example, ‘hold the cup tight – good, well done’, rather than ‘don’t drop the cup’
- Offer a brief explanation of why behaviour is not acceptable and a clear indication of what is preferred. For example: ‘If you shout it’s really hard for me to hear what you want to say. I want to be able to hear you, so please talk in an ordinary voice’.
- Help child to list and think about all the things they have done that they feel proud of.
- Help child to think about times, events, occasions when they felt valued and special. Use photos and other mementos to record these events.
- List alongside child, all the things that make you feel proud of them. Can include acceptance of limitations (e.g. a time when the child tried but did not succeed at something, was able to accept loosing etc.).
- Encourage child to draw, paint, make a clay model or play in music how it feels when they feel good about herself. Do the same for yourself.
- Suggest that child lies on the floor, draw round the outline of the child’s body. Encourage the child to make a positive statement about different parts of herself (I’ve got shiny brown hair, a pretty T shirt etc.) and write or draw these onto the figure. Take this at the child’s pace and ensure the child feels comfortable with the statement made.
- As a family group, suggest that each person in the family writes down one good thing about all other family members, so that each child gets given a set of positive things about themselves.
- Make a poster with the child of ‘best achievements’.
- Ask child to teach you something that he is good at – such as a computer game or a joke.
- Buy a small treat and place it in the child’s bedroom as a surprise.
- Discover and support activities and interests that the child enjoys and can be successful in. May need active support (liaison with club leader, becoming a helper at the club etc.).
- Use dolls, toys, games and books that promote a positive sense of the child’s ethnic, religious and cultural background.
- Ensure that the child’s ethnic, religious and cultural background is valued and celebrated within the household.
- Model the acceptance of difference in words and behaviour.
- Model a sense of pride in self and surroundings.
- Model within the family that it is OK not to be perfect, that no one is good at everything but everyone is good at something.
(Source: Providing a Secure Base, Gillian Schofield and Mary Beek, University of East Anglia, Norwich, UK)
Co-operation – approaches for helping children to feel effective – and be co-operative
N.B. It is important to choose only activities that the child is likely to accept and enjoy.
- Find individual activities that the child enjoys and that produce a clear result. For example, give the child a disposable camera to use on holiday or on a day out, help them to get the photos developed and give them a small album for the results.
- Within the house and garden, minimise hazards and things that child cannot touch and keep ‘out of bounds’ areas secure so that the child can explore without adult ‘interference’ when he is ready to do so.
- Suggest small tasks and responsibilities within the child’s capabilities. Ensure recognition and praise when achieved. If they become an issue, do them alongside the child – a chance to show availability.
- Introduce toys where the action of the child achieves a rewarding result. For example, pushing a button, touching or shaking something.
- Make opportunities for choices. For example, allow child to choose the cereal at the supermarket, a pudding for a family meal, what to wear for a certain activity.
- Ensure that daily routines include time to relax together and share a pleasurable activity.
- Respond promptly to child’s signals for support or comfort or reassure an older child that you will respond as soon as possible. For example ‘I must quickly finish what I am doing and then I will come and help you straight away’.
- Do not try to tackle several problem areas at any one time. Set one or two priorities and work on them gradually until there are sustained signs of progress. Ensure that these are acknowledged.
- Use co-operative language wherever possible. For example ‘Would you like to come and have a sandwich after you’ve washed your hands’, rather than ‘Wash your hands before you eat your sandwich’.
- Find shared activities that the child enjoys and that produce a clear result. For example, baking cakes.
- Introduce games. State clearly when you have had enough and suggest alternative activity.
- Seek opportunities for the child to co-operate with other children – you may need to be present so that this is managed successfully.
- Help the child to identify a target that they would like to achieve, do, change etc. Settle on one where something done now will make a difference. Discuss what the young person can do and negotiate simple, relevant and achievable steps that they can take. When agreed, draw a simple staircase and write one task in each of the bottom steps of the staircase. For example, if the target is ‘go to see Manchester United play at home’, steps might be – use internet to find out dates of home games this season, settle on suitable date and put on calendar, find out train times, etc. Set a time to review progress and think about further steps needed.
(Source: Providing a Secure Base, Gillian Schofield and Mary Beek, University of East Anglia, Norwich, UK)
Family Membership – approaches for helping children to belong
N.B. It is important to choose approaches for helping children to belong that are suitable for the individual child and the plan for this child.
Belonging in an adoptive family, foster family or residential group
- Explain to the child from the beginning how the family/group works – its routines and expectations, its choice of food and favourite television programmes – so that the child can see how to fit in.
- Adapt those routines where possible and reasonable to accommodate the child’s norms and help the child feel at home e.g. meal times or bedtime.
- Have special places for the child in the home e.g. a hook for the child’s coat; a place at the table; the child’s name on the bedroom door or in fridge magnets on the fridge; bedding and bedroom decoration (posters etc.) that reflect the child’s age and interests.
- Promote family/group mealtimes and activities (e.g. going bowling) where the child can feel fully accepted as part of the family/group.
- Ensure extended family members and friends/all staff members welcome the child and treat the child as one of the family/part of the group.
- Have photographs of the child and of the child with the foster or adoptive family or residential caregivers on display – alongside photographs of other children who have lived in the foster or adoptive family or residential unit and moved on/grown up.
- Use memory and experience books of events and feelings about events during the child’s stay to build a family story to help the child be able to reflect on the meaning of family/group life and, if the child moves on, to take home to the birth family or to a new placement.
- Make sure the school knows (and the child knows that the school knows) that you are the family/residential unit caring for the child and need to be kept informed of any concerns but also of things to celebrate.
- Plan family/group life and talk about plans that will include the child, even if this is just an expectation that they will all go swimming together next week.
- Belonging to the birth family when separated.
- Develop or build on an existing life story book that contains information, pictures and a narrative that links the child to birth family members and birth family history. Ensure that it includes key documents e.g. copy of birth certificate, provides a full and balanced picture (see also Chapter 12) and is nicely presented, robust, valued and cared for. Even children who return to birth families benefit from making sense of complex family histories and their place in the family.
- Have photographs of the birth family where the child would most like to put them, e.g. bedroom or living room.
- Ensure that conversations about the birth family happen appropriately and are carefully managed within the family/group, so that the child does not have to make sense of negative, contradictory or idealised ideas about the birth family.
- Where direct or indirect contact is occurring, be actively involved in planning and facilitating contact so that the child’s welfare is paramount and contact promotes security as well as roots and identity.
- Managing memberships of more than one family.
- Adults need to demonstrate their own flexibility about children’s family memberships and what they might mean to the child.
- Both informally and in a planned way, talk with the child about the benefits and the challenges of having more than one family and help the child to understand and manage these relationships.
- Find models around the child of children who manage multiple families e.g. in friends’ families, on television, in books.
- Help the child think about/talk about the inevitability of mixed feelings.
- Watch for possible pressure points e.g. Mother’s Day, Father’s Day, Christmas, and find ways of indicating (where appropriate) that it is OK to give cards to more than one parent or to choose one rather than the other at different times.
- If necessary and with the child’s permission talk to the teacher about family issues that may disturb the child if raised in class, i.e. help others outside immediate family circle be aware of the child’s task in managing their multiple loyalties/families.
(Source: Providing a Secure Base, Gillian Schofield and Mary Beek, University of East Anglia, Norwich, UK)
Allowing children to take risks
As well as promoting the safety and welfare of children in their care, foster parents have to support and encourage children to take appropriate risks as part of normal growing up and to learn from their mistakes. This includes allowing children to participate in every day rough and tumble activities and physical sports, as well as permitting them the opportunities to participate in organised activities through school, such as outward bound weeks, canoeing and kayaking etc.
Decisions about what is an ‘appropriate risk’ will often be child specific and will relate to the child or young person’s previous experiences, age, developmental stage, confidence and other attributes. Foster parents should consult about and review such matters regularly with their supervising social worker and ensure that they are reflected in the placement plan. The principle is that children and young people in foster care should have the same opportunities as other children to try out new activities, take risks and learn from them. Foster parents should feel supported in helping children to do this and not feel that they cannot agree to anything.
Discipline and Sanctions
Disciplining children to develop an awareness of danger and respect for the rights, needs and feelings of others, as well as helping them to develop appropriate self-control, is a daunting responsibility for all parents and caregivers. Most parents use the experiences of their own childhood and family life as a basis for their approach to discipline.
Secure base theory and research into foster care tells us that foster parents need to be sensitive and try to identify and understand patterns of thinking and behaviour that reflect a child’s coping or defensive strategies. The focus should always be on helping the child to express and talk about their feelings and the foster parent must have the capacity to ‘stand in the shoes of the child’, before approaches to discipline are routinely adopted. This caregiving cycle begins with the child’s needs and behaviour but then focuses on what is going on in the mind of the caregiver. How a foster parent thinks and feels about a child’s needs and behaviour will determine his or her caregiving behaviours. The foster parent may draw on their own ideas about what children need or what makes a good parent from their own experiences or from what they have learned from training. The caregiving behaviours that result convey certain messages to the child. The child’s thinking and feeling about themselves and other people will be affected by these messages and there will be a consequent impact on his or her development. This process is represented in a circular model, the caregiving cycle, which shows the inter-connectedness of caregiver/child relationships, minds and behaviour, as well as their ongoing movement and change.
There is also a level of prescription about use of discipline and sanctions for fostered children and foster parents need to be aware of what the expectations are upon them.
Research indicates that looked after children on average are involved earlier and more often than other young people with the police and criminal justice system. Fosterplus is committed to trying to minimise the need for police involvement in dealing with challenging behaviour, and we wish to avoid criminalising foster children unnecessarily. You can contact your supervising social worker and/or our out of office hours service to discuss any concerns or issues that you may have concerning a young person’s behaviour.
Acceptable sanctions and punishments
Wherever possible, foster parents should use constructive dialogue with the child or guide them away from a confrontational situation. The aim at all times is to try to think flexibly about what the child may be thinking and feeling and to reflect this back appropriately to the child.
Foster parents should also have an understanding of their own emotional response to a confrontation or threat, and know when to withdraw, concede or seek help. Where sanctions are used, it is important that they are:
- Relevant for the child and related to his or her care plan, age and circumstances.
- Realistic and sensitive.
- Understandable for everyone in the household.
- Used sparingly.
- Time limited.
- Justified.
- Follow the behaviour as quickly as possible.
- Follow good practice in the care of children/young people.
- Have been discussed during the placement planning meeting.
- Recorded by the foster parents on the child’s CHARMS case record.
Sanctions/punishments may include:
- Loss of/withdrawing privileges – e.g. loss of staying up late on a special night of the week, or visiting friends. This can help the young person understand that the unwanted behaviour will not be tolerated.
- Going to bed early – This can be used alongside other methods of control, and is particularly useful when it is linked to behaviour in which the young person has been late home, been disruptive at bedtime etc. Young people should not be sent to bed more than one hour before their normal bedtime.
- Paying towards damages – Young people could be expected to pay a portion of their pocket money regularly until they have made amends, or made an agreed contribution towards damage. The whole of a child’s pocket money must never be taken. They must always have some money that is their own each week. Any money stopped for reparation is clearly recorded by the foster parent in their diary sheets and should have prior agreement of the child’s supervising social worker and local authority social worker.
- Doing extra jobs – Like tidying the living room each day for a week if they have been responsible for creating a messy environment for others.
- Grounding for a time – This should be used sparingly and linked to the behaviour which has been unacceptable e.g. the young person may have damaged trust by not returning home at the agreed time.
- No television or treat – A difficult punishment if it means that others in the family will also lose out, but possible to achieve if a young person has a particularly favourite programme, and it is possible to use another room while others watch TV.
- Withdrawing attention – This can be an effective means of decreasing unwanted behaviour in children by not giving any attention to the unwanted behaviour. Care should be taken to ensure that this behaviour would not result in the child being placed in any danger. Foster parents should also try to ensure that they do reward positive behaviour. Withdrawing attention should be for short impact periods only. A strategy could be to tell the child that if they sit quietly for ten minutes, then it will be time for a game.
- Time out – This gives everyone the opportunity to reflect on what has happened. Time out should only be used for very short periods, particularly if the child is young. Telling them to sit on a chair just outside the room that the foster parent is in for five minutes can constitute time out. Bedrooms where children have toys should not be used for time out.
- Verbal disapproval – A raised voice, or different tone, can signal to a child that the adult is displeased. Foster parents need to make clear to the child that it is the behaviour that is disliked, not the child. Children should not be reprimanded in public if possible.
- Increased supervision – Young people like freedom, and knowing that someone is taking a keener interest in their activities can help them re-consider how they behave.
- Contracts – These can be particularly useful for older children, or where a young person wants to work towards something. Contracts are a sophisticated measure which must be discussed with the Supervising social worker in the first instance.
Unacceptable measures of control and discipline
Unacceptable sanctions include those that intentionally or unintentionally humiliate a child or young person, cause them to be ridiculed, or have been experienced by a child or young person under different circumstances at home, and which may evoke past painful and traumatic memories.
Foster parents should never threaten to end a placement as a punishment for the child who is living with them. They may have previously experienced this threat being carried out in their own family, and it can seriously damage relationships in the foster home.
There are a number of unacceptable methods of control that are forbidden by legislation. These include:
- Corporal punishment – any intentional application of force as punishment, including smacking, slapping, punching, rough handling, grabbing and throwing missiles.
- Deprivation of food and drink.
- Restriction on visits to or communication with parents, relatives, social worker, children’s guardian, solicitor.
- Any requirement that a child wears distinctive or inappropriate clothes.
- Use or withholding of medication or dental treatment.
- Locking a child in a room or building. (This does not include time out in a child’s unlocked bedroom, the use of which should be limited and used in a positive way).
- Intentionally depriving the child of sleep.
- Imposing fines other than for compensation or repayment.
- Intimate physical examination of a child.
There are other unacceptable methods of control which are not forbidden by legislation, but which we would not accept as good practice, including:
- Keeping a child in isolation because of their behaviour – if isolation is necessary because of other reasons, it must only be with close adult supervision.
- Excessive use of sending a child to bed early as a punishment – bedtime should be a pleasant experience, and a child’s day should not end in an unsatisfactory way.
- Bribery or threats – this should not be confused with encouragement and praise as an incentive to promote appropriate behaviour.
Physical intervention by foster parents
Physical intervention on children should only be used in exceptional circumstances, where it is the only appropriate means to prevent likely injury to the child or other people, or likely serious damage to property.
In the event of a serious incident (e.g. accident, violence or assault, damage to property), foster parents should take what actions they deem to be necessary to protect children and themselves from immediate harm or injury. They must notify the agency immediately afterwards.
If there is a risk of serious injury, harm or damage to property, foster parents should not use any form of physical intervention, except as a last resort to prevent themselves or others from being injured, or to prevent serious damage to property. If any form of physical intervention is used, it must be the least intrusive necessary to protect the child, foster parent(s) or others. At no time should foster parents act unless they are confident of managing the situation safely, without escalation or further injury.
The agency will endeavour to deal with as many as possible of the challenges that are involved in caring for children without recourse to the Police, who should only be involved in two circumstances:
- An emergency necessitating their immediate involvement to protect the child or others; or
- Following discussion with the supervising social worker, Service Manager, Head of Operations, or the Out of Hours Manager (outside office hours).
If any serious incident occurs or the Police are called, the supervising social worker, Service Manager, Head of operations or Out of Hours must be notified without delay. They will then notify the relevant social worker(s) and arrange for a full report to be made of the incident and the actions taken.
Where there is significant evidence of patterns of violent or dangerous behaviours, the supervising social worker will liaise closely with the child’s social worker and foster parent, in order to agree how such behaviours should be best managed.
Recording of sanctions
Foster parents should record, in detail, any sanctions that they have used with a child or young person, including why they were used, what led up to the incident, an account of the behaviour/incident, and the consequences/outcome of the incident. Any triggers to the situation for the child/young person should be noted.
The information should be recorded on the carer log. Please inform your local office as soon as possible, by telephone, of any incident that you have recorded in CHARMS.
Where foster parents have used sanctions that were not previously agreed, it is particularly important that they carefully record the events and the sanctions used for discussion later with their supervising social worker, the young person, and where appropriate, their parent. The appropriateness of the actions should be discussed, and alternative action explored for the future if necessary.
The use of sanctions should be monitored for their effectiveness by the foster parent and supervising social worker. Significant use of an inappropriate sanction, or continued use of inappropriate sanctions may be deemed as a child protection issue and be investigated accordingly.
Suicide and self-harm
Looked after children are at greater risk of committing suicide than other young people. We must treat all histories and incidences of suicidal thoughts, suicidal attempts and self-harm seriously and not be tempted to deny or minimise their significance. We must not allow ourselves to be over optimistic about a child’s self-harming and assume that someone with a history of self-harming will not also attempt suicide. We must also be alert to recognising less common forms of self-harm such as refusal to take prescribed medication such as insulin. Dealing with a child who self-harms can be very frustrating, anxiety provoking and stressful. The trauma of the child can be transferred to the professional, who may react in a number of unhelpful ways, including intervention paralysis, drift or overreaction.
An intervention plan must be agreed with the local authority and foster parents must not act without the agreement and full knowledge of their supervising social worker. This area is one where individual, subjective thresholds play a very significant part in deciding whether we are concerned enough to intervene. The facts, history and risks must be established first, before decisions are reached about whether intervention or non-intervention is appropriate. Where there are differences in personal thresholds amongst professionals, we must work for consensus. When this cannot be achieved, we must establish and record clear accountability and decision making.
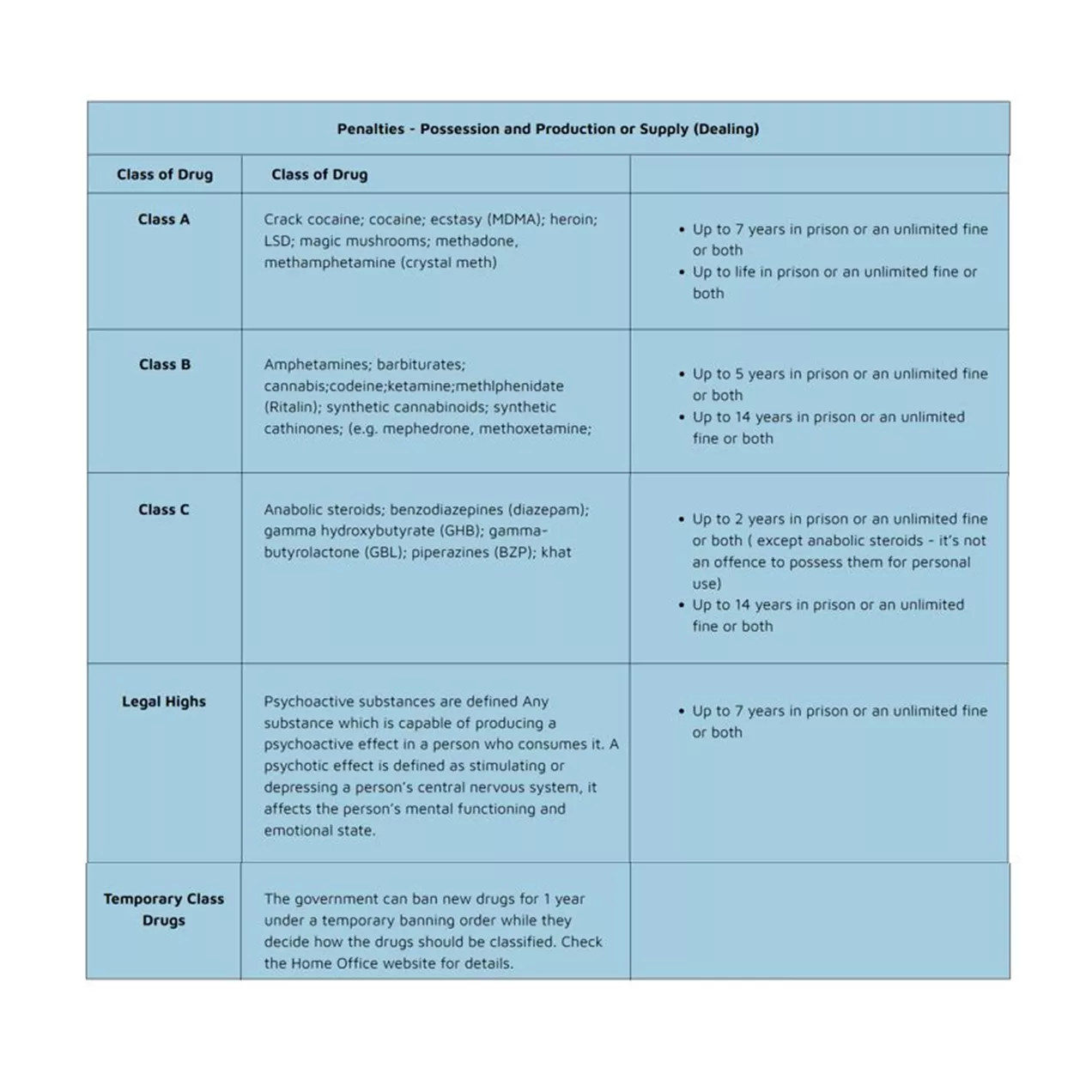
Confiscation of dangerous, illegal or unacceptable items
Any alcohol, illegal drugs, substances, solvents or weapons found in the possession of any child or young person should be confiscated by the foster parent and reported to, and handed in to, the child’s social worker or supervising social worker. Possession of such items should be considered as a significant incident and reported immediately to the supervising social worker or out of hours service. Fosterplus may seek advice regarding legal issues to assist everyone in determining the right way forward.
If foster parents discover that a child or young person in their care has taken illegal drugs, they must immediately contact their supervising social worker, or use the out of hours telephone support number to seek advice and action. It is not appropriate for foster parents to try and deal with this situation on their own.
Safeguarding Children / Child Protection
What is child abuse?
It is generally accepted that there are four main forms of abuse. The following definitions are taken from National Guidance for Child Protection in Scotland 2014
Physical Abuse
Physical abuse is the causing of physical harm to a child or young person. Physical abuse may involve hitting, shaking, throwing, poisoning, burning or scalding, drowning or suffocating. Physical harm may also be caused when a parent or carer feigns the symptoms of, or deliberately causes, ill health to a child they are looking after. For further information, see the section on Fabricated or induced illness.
Emotional abuse
Emotional abuse is persistent emotional neglect or ill treatment that has severe and persistent adverse effects on a child’s emotional development. It may involve conveying to a child that they are worthless or unloved, inadequate or valued only insofar as they meet the needs of another person. It may involve the imposition of age – or developmentally – inappropriate expectations on a child. It may involve causing children to feel frightened or in danger, or exploiting or corrupting children. Some level of emotional abuse is present in all types of ill treatment of a child; it can also occur independently of other forms of abuse.
Neglect
Neglect is the persistent failure to meet a child’s basic physical and/or psychological needs, likely to result in the serious impairment of the child’s health or development. It may involve a parent or carer failing to provide adequate food, shelter and clothing, to protect a child from physical harm or danger, or to ensure access to appropriate medical care or treatment. It may also include neglect of, or failure to respond to, a child’s basic emotional needs. Neglect may also result in the child being diagnosed as suffering from “non-organic failure to thrive‟, where they have significantly failed to reach normal weight and growth or development milestones and where physical and genetic reasons have been medically eliminated. In its extreme form children can be at serious risk from the effects of malnutrition, lack of nurturing and stimulation. This can lead to serious long-term effects such as greater susceptibility to serious childhood illnesses and reduction in potential stature. With young children in particular, the consequences may be life-threatening within a relatively short period of time.
Sexual abuse
Sexual abuse is any act that involves the child in any activity for the sexual gratification of another person, whether or not it is claimed that the child either consented or assented. Sexual abuse involves forcing or enticing a child to take part in sexual activities, whether or not the child is aware of what is happening. The activities may involve physical contact, including penetrative or non-penetrative acts. They may include non-contact activities, such as involving children in looking at, or in the production of indecent images or in watching sexual activities, using sexual language towards a child or encouraging children to behave in sexually inappropriate ways (see also section on child sexual exploitation).
Peer on Peer Abuse
The term ‘peer on peer abuse’ relates to various forms of abuse, where all parties involved are under the age of 18 years. The abuse can include violence and criminal activity, harmful sexual behaviour, sexual exploitation, relationship abuse and bullying (including cyberbullying) and is harmful to both the victim and the perpetrator due to their status as children.
The victims of peer on peer abuse are both male and female and particularly vulnerable groups include those with disabilities and those who represent minority groups (e.g. on basis of sexuality, race or religion). Peer on peer abuse is often a feature of gang activity, and a victim might experience a combination of different abuses and have multiple support needs.
Where does peer on peer abuse occur?
Young people in foster care might experience abuse from their peers:
- Within the foster home
- At school
- At clubs/social activities
- On public transport/walking to school
Agency response
Foster parents and agency staff need to be alert to the signs of peer on peer abuse and be familiar with agency policies to ensure a swift and appropriate response. Young people’s risk assessments should identify key concerns and safeguarding measures both for use within the home and community.
- Being aware of, and managing bulling:
Bullying is defined as “behaviour by an individual or group, usually repeated over time, which intentionally hurts another individual or group either physically or emotionally.” Bullying behaviour can include name calling, hitting, pushing, spreading hurtful and untruthful rumours, taking belongings, inappropriate touching or excluding someone from a social group. Young people might be targeted as a result of their race, religion, sexuality or disability and bullying might take place online. This is known as ‘cyberbullying’. The Anti-Bullying Alliance has an excellent interactive online resource for parents and foster parents to raise awareness of bullying issues, https://anti-bullyingalliance.org.uk
- Gangs awareness
Young people can be exploited physically and/or sexually by a gang or group of young people. Gangs (mainly comprising young men and boys aged 13-25 years) are typically involved in various forms of criminal activity including violence with knives and guns, robbery and intimidation, exposing both gang members and targets to harm. Gangs are characterised by their identifiable markers including territory, name and clothing, while other groups without specific gang characteristics exist within the community and online to exploit young people, often sexually.
Click here to view a helpful Government guide to gang activity for parents and carers >
- CSE awareness
The sexual exploitation of young people by adult perpetrators has been well publicised with recent prosecutions of adult males in Rotherham and Rochdale. Young people can also be sexually exploited by older young people and this is reflected in the most recent definition:
CSE “occurs when an individual or group takes advantage of an imbalance of power to coerce, manipulate or deceive a child or young person under the age of 18 into sexual activity”
CSE always involves in imbalance of power and victims might not be aware of the exploitation, perceiving the relationship as loving. https://www.kscmp.org.uk/guidance/exploitation
- Youth produced sexual imagery (“sexting”)
The sharing of nude images online between young people is not always intentionally harmful but has the potential to harm if there are elements of coercion, bribery and/or blackmail involved. Young people can feel pressured to send nude images and once images have been shared they lose control over them; the image can be copied and shared indefinitely. The law prohibits the taking, possessing and sharing of ‘indecent images of children’ which includes nude images shared between young people, if the subject of the image is under 18 years of age. Young people who are involved in this behaviour can therefore need support with both the emotional impact of image sharing as well as possible police investigations.
CEOP has a helpful online guide for parents and carers >
Resources for young people
Childline: 0800 11 11 or find out about the “For Me” app at https://www.childline.org.uk/toolbox/for-me/
National Guidance for Child Protection in Scotland 2014
The Scottish Government’s guidance on inter-agency working to safeguard and promote the welfare of children can be downloaded at:
https://www.gov.uk/government/publications/working-together-to-safeguard-children–2
Staff and foster parents who are in positions of trust
Legislation states that it is a criminal offence for adults who are in positions of trust to commit sexual acts (including inappropriate touching), or have sexual relationships, with young people between the ages of 16 to 18 years in their care (even if the young person initiates or consents to the sexual activity). This legislation also applies to people over the age of 18 years if they are deemed to be ‘vulnerable’. The legislation is primarily intended to protect young people where a relationship of trust with an adult looking after them exists.
A position of trust can be broadly defined as a relationship in which one party is in a position of power or influence over the other by virtue of their work or nature of their activity. A young person is vulnerable to exploitative contact or relationships irrespective of their chronological age. Some work roles such as Social Worker or foster parent are defined within the legislation as being positions of trust. Positions of trust may also be created by virtue of the nature of the adult’s contact with a young person; for example a relative of a foster parent caring for a fostered child for short periods during the daytime would be in a position of trust. Adult members of the foster parent’s household including sons and daughters may also be seen to hold positions of trust in some circumstances.
Allegations or complaints would be subject to the procedures defined in the Scottish Government guidance Managing Allegations against foster parents and approved Kinship Carers (2013). Fosterplus’s Child Protection procedures take account of this guidance. Conviction of criminal charges under this legislation may lead to a custodial sentence and a referral to the Disclosure and Barring Service.
If a foster parents feels sexually attracted to a young person they care for, they have a personal and professional responsibility to inform their supervising social worker. The social worker must consult with their Registered Manager and the Quality Assurance and Safeguarding Team as to the appropriate actions to safeguard the young person concerned (including moving the young person to a different placement).
Disclosure Scotland Checks
Applicants to foster and all people aged 16 or over living or regularly visiting their household will be asked to complete the disclosure forms and produce the necessary identification. There are different levels of checks the highest being PVG (Protecting Vulnerable Groups) and depending on the role of the individual different checks will apply. These will then be sent to the Disclosure Scotland Service by the fostering service. Disclosure Scotland checks are not transferable, so copies of checks carried out by other agencies or for other posts cannot be accepted. Checks will be updated at least every three years.
Child Sexual Exploitation (CSE)
Child sexual exploitation takes different forms – from a seemingly ‘consensual’ relationship where sex is exchanged for attention, affection, accommodation or gifts, to serious organised crime and child trafficking. Child sexual exploitation involves differing degrees of abusive activities, including coercion, intimidation or enticement, unwanted pressure from peers to have sex, sexual bullying (including cyber bullying), and grooming for sexual activity. Child sexual exploitation is not gender specific. There is increasing concern about the role of technology in sexual abuse, including via social networking and other internet sites and mobile phones. The key issue in relation to child sexual exploitation is the imbalance of power within the ‘relationship’. The perpetrator always has power over the victim, increasing the dependence of the victim as the exploitative relationship develops.
Many children and young people are groomed into sexually exploitative relationships but other forms of entry exist. Some young people are engaged in informal economies that incorporate the exchange of sex for rewards such as drugs, alcohol, money or gifts. Others exchange sex for accommodation or money as a result of homelessness and experiences of poverty. Some young people have been bullied and threatened into sexual activities by peers or gangs which is then used against them as a form of extortion and to keep them compliant.
Children and young people may have already been sexually exploited before they are referred to children’s social care; others may become targets of perpetrators whilst living at home or during placements. They are often the focus of perpetrators of sexual abuse due to their vulnerability. All staff and foster parents should therefore create an environment which educates children and young people about child sexual exploitation, involving relevant outside agencies where appropriate. They should encourage them to discuss any such concerns with them, another member of staff, or with someone from a specialist child sexual exploitation project, and also feel able to share any such concerns about their friends.
As an agency, Fosterplus has a strong commitment to learning and development and believes that this is an important part of exploring the subject of Child Sexual Exploitation. Core training has been specifically designed by the agency and all foster parents, staff, panel members and volunteers are expected to attend this course which explores the meaning of Child Sexual Exploitation and working with children who have been or are at risk of being sexually exploited.
Child Sexual Exploitation Risk Assessments
These assessments are completed in addition to ‘Safeguarding Risk Assessments’ where there is an indication or concern that the child or young person is at risk of Child Sexual Exploitation (CSE). The CSE Risk Assessment provides a method of establishing the level of risk the young person is at of being a subject of Child Sexual Exploitation. This risk assessment focuses specifically on the known vulnerabilities and indicators of Child Sexual Exploitation. However, these assessments must be considered alongside regular Safeguarding assessments as each should inform the other.
Female Genital Mutilation
Female genital mutilation (FGM) is a collective term for procedures which include the removal of part or all of the external female genitalia for cultural or other non-therapeutic reasons. The practice is medically unnecessary, extremely painful and has serious health consequences, both at the time when the mutilation is carried out and in later life. The procedure is typically performed on girls aged between 4 and 13, but in some cases it is performed on new-born infants or on young women before marriage or pregnancy.
FGM has been a criminal offence in the U.K. since the Prohibition of Female Circumcision Act 1985 was passed. The Female Genital Mutilation Act 2003 replaced the 1985 Act and made it an offence for the first time for UK nationals, permanent or habitual UK residents to carry out FGM abroad, or to aid, abet, counsel or procure the carrying out of FGM abroad, even in countries where the practice is legal.
The rights of women and girls are enshrined by various universal and regional documents which highlight the right for girls and women to live free from gender discrimination, free from torture, to live in dignity and with bodily integrity.
Where a foster parent has concerns about the welfare and safety of a child or young person in relation to Female Genital Mutilation they should immediately inform their supervising social worker.
Trafficked Children
Who are trafficked children?
Trafficked children are likely to be children who arrive in the country as unaccompanied children or asylum seekers. They are brought into the country for the purposes of adult exploitation, which could include prostitution or sexual abuse, forced or/and cheap labour, slavery or servitude, financial or benefits fraud, and being used as drug ‘mules’. Such children may be unaware that they have been brought into the country for such purposes, others may be too frightened to tell, whilst a few may be aware but compliant.
Identifying trafficked children
Unaccompanied children arriving in the country are screened by the immigration authorities at the point of entry. Some children will have only vague arrangements as to their future care or the immigration authorities may have concerns about the adults who have been identified as their future foster parents. Such children are likely to be placed with foster parents for at least a short period pending the outcome of further investigations. These children are at particular risk of adult exploitation, but will rarely disclose their experiences directly to a foster parent. However, children are likely to show patterns of behaviour and activity which may indicate that the child is the subject of adult exploitation. These include:
- Does not appear to have any money but does have a mobile phone when first placed.
- Receives unidentified/unexplained phone calls.
- Possesses money/goods not accounted for.
- Has a prepared story and appears to have been coached or rehearsed in recounting how they arrived in the country.
- Shows signs of physical or sexual abuse or sexually transmitted disease or pregnancy.
- Has unexplained absences from the foster parents’ home or goes missing.
- Unidentified adults loitering outside or near foster parents’ home.
- Has significant sums of money which are not adequately accounted for.
- Acquires expensive clothes, mobile phones etc. without plausible explanation.
- Possesses keys to unidentified premises.
- Truancy.
- Observed entering or leaving cars driven by unknown adults.
- Found in areas the child has no known links with.
- Inappropriate use of internet and forming online relationships with adults.
These indicators are not a definitive list but provide a guide to alert foster parents that a child might be ‘trafficked’.
Safeguarding children at risk of being trafficked
When unaccompanied children are first placed with foster parents, the local authority should undertake a risk assessment of the child and should plan for the possibility that the child may be ‘trafficked’. If and when a foster parent feels that there is evidence that the child may be ‘trafficked’, then they should report their concerns to their supervising social worker who will liaise with the local authority social worker. The local authority will decide whether the concerns or evidences warrant the implementation of formal child protection procedures.
Children Missing from Care
Children at risk of going missing
At the point a child is placed with foster parents there should be a Risk Assessment completed, which will include any specific factors that may increase the possibility of the child going missing. Any identified risk factors should then be addressed in a way that will reduce the possibility of a child going missing. For example, clear arrangements for contact between a foster child and his/her birth family may decrease a child’s level of anxiety about seeing his/her family and therefore their likelihood of running away.
In addition to the Risk Assessment, the foster parent and/or supervising social worker should complete a record detailing information such as the child’s height, distinguishing features etc. which can be given to the Police if the child is actually reported as missing. This may include a photo, which should only be taken with the child’s agreement and those who hold parental authority.
The placement plan should define the circumstances in which a child is authorised to be absent from a foster parent’s home. For example, it could record that an older teenager may stay with a close friend one night every two weeks on an on-going basis, without identifying the specific dates. The placement plan should detail who has authority to agree such an arrangement on each individual occasion e.g. the foster parent, and whether the foster parent should inform each absence to the Fosterplus OOH service. These arrangements would be viewed as authorised absences rather than unauthorised absences or a missing child.
Foster parents should know when to try to prevent a child or young person leaving the home and should do so through dialogue, but they should not physically intervene to try to restrain any child should they be intent on leaving, or in any other circumstances, unless it is necessary to prevent injury to the child or others, or serious damage to property. No physical intervention may be excessive or unreasonable.
What to do when a child or young person is missing
In order to avoid any confusion, Fosterplus foster parents should, in all instances where a child is absent from their care without permission, contact their supervising social worker or their Service Manager during normal working hours, or the OOH service at evenings or weekends, to report the child’s absence.
The supervising social worker will ascertain whether any further steps can be taken to identify the child’s whereabouts e.g. phoning the child’s mobile phone number, family or friends, visiting the address the child claims to be at. It may be that the foster parent is the best placed person to visit addresses (subject to any safety issues) as – in terms of the Secure Base Model – this is a powerful demonstration to the child/young person of the foster parent’s availability and that the child has a place – i.e. ‘belongs’ – in their foster family.
The supervising social worker may exercise a professional judgement in allowing a child some time to return to their foster parents before taking any further action; for example, if the child has informed their foster parent they been delayed because they are waiting for a bus.
Reporting the child as missing
When it is evident that a child’s whereabouts are unknown, the supervising social worker (or Out of Hours worker) will advise the foster parent to report the child as a Missing Child immediately, without the need to consult first with the child’s placing authority. The supervising social worker will then inform the placing authority as soon as possible.
The supervising social worker/duty worker will always inform the placing authority of a child’s absence. In this situation, after consultation with the local authority, a decision will be reached as to whether the child should be reported as a Missing Child to the Police and the supervising social worker/duty worker will advise the foster parent accordingly. In order to avoid any possible misunderstandings, the person reporting the child’s absence to the Police should always emphasis why a child may not be safe, even if the child’s whereabouts may be known.
The foster parent is normally the person best positioned to report a foster child as a Missing Child to the Police. They will be visited by the Police for the purpose of collating information about the child and their possible whereabouts. Copies of any relevant forms and photos should be made available to the Police. Depending on the circumstances, the Police may search the foster parent’s home and garden to make sure the child is not hiding on the premises.
Most missing children are found quickly, but occasionally children may be missing for substantial periods of time or may repeatedly go missing. Local authorities are required to have mechanisms in place to ensure all agencies and services remain pro-active in identifying the child’s whereabouts and safe return.
When a Missing Child is Found
The Police are the people most likely to find a Missing Child and may return the child directly to the foster parent’s home or take the child to a local Police Station. A Police Station may be regarded as simply a safe place for the child to be kept whilst awaiting collection by the foster parent or social worker. Alternatively, the child may have been taken to the Police Station because the Police have reason to believe the child has been involved in some form of criminal activity.
The age of criminal responsibility in Scotland is a significant and complex policy area, which raises sensitivities due to the potential for rare, serious cases involving young children. Children under 12 cannot be prosecuted in court in Scotland, but those aged 8 and over can be referred to the children’s hearings system on offence grounds.
The minimum age of prosecution was set at 12 through changes in the Criminal Justice and Licensing (Scotland) Act 2010. That change has worked well, though it has not ended discussion about the age of criminal responsibility. There is ongoing consultation on this.
How should foster parents respond when a Missing Child is found?
In all instances when a child is found after being reported as absent they should be given the opportunity to discuss their reasons with another professional in a ‘Return Interview’. This interview should take place, if possible, before the child actually returns to their foster parent, but certainly within 72 hours of the child returning. Guidance is that this interview should be conducted by a person ‘who is independent of their placement’. This person might be the child’s local authority social worker or an independent person or advocate.
The supervising social worker responsible for the child’s placement should consult with the child’s social worker as to who should conduct this interview. If the child’s social worker is unable to identify a suitable person, then the supervising social worker may conduct this interview themselves or commission someone else suitable to do it and will provide written feedback to the child’s social worker.
Children run away for a variety of reasons, but often because they are confused or unhappy about something. Though the reason may sometimes seem very trivial to the foster parents, at the time the child ran away it was the only way they felt they could deal with their confusion or unhappiness. They may not have got very far away, before they realised that there were other ways of dealing with the problem. They may feel very embarrassed and so coming home may be difficult and they will need an understanding welcome.
Whilst the child is missing, foster parents will often be trying to understand why and perhaps blaming themselves for what has happened. When the child absents themselves frequently, foster parents and their families can feel physically tired from lack of sleep and worry, dispirited and resentful at the child’s apparent disregard of their needs and feelings. Sometimes in such circumstances, foster parents may feel that the process of reporting a child as missing is long and unproductive. When the child returns, they may be filled with a mixture of anger and relief. Negative feelings need to be acknowledged and managed and foster parents should expect help and support from the child’s social worker and their supervising social worker, so that they will be in a position to be helpful to the child, when they return.
Where an individual goes missing for a long period of time or very regularly, the child, responsible authority, fostering service staff and foster parents should meet together to decide what further action should be taken to help and protect the child.
Recording when a child goes missing
Fosterplus maintains written records on a child’s CHARMS case record of when a child goes missing. These include logs and incident reports submitted by and detailing action taken by foster parents, the circumstances of the child’s return, any reasons given by the child for running away from the foster home and any action taken in the light of those reasons. It is a requirement to notify the local authority for the child and the Care Inspectorate and Fosterplus records this using the progress action ‘Notifiable Event – Child missing from placement (whereabouts unknown)’.
This information is shared, where appropriate, the child’s parents.
Payments to foster parents when a child is missing
Payments may continue when a child absconds until the placement has formally ended, as long as the Fosterplus Head of Operations is satisfied that the situation is being monitored closely and is kept informed. Payments will not continue indefinitely. They are subject to monitoring and review. There are tight time limits, as the placing authority may decide to terminate a placement if a child is absent for more than a few days.
Bullying
Anti-Bullying Procedure
Fosterplus considers that any bullying behaviour is unacceptable and should not be tolerated. Our policy in relation to bullying can be downloaded from
CHARMS/Download.
We try to ensure a culture in Fosterplus that regards any form of bullying as totally unacceptable. Foster parents and staff should be able to recognise and deal with any indications or incidents of bullying, act proactively and intervene positively, engaging with those bullying as well as those being bullied. Children who are bullied should be supported and those who bully given help and guidance to prevent them continuing to do so.
What is bullying and how to respond?
Bullying can include the following types of behaviour:
- Name calling and teasing, including taunts about sexual orientation and race.
- Gestures, taunting and mocking.
- Making offensive comments.
- Malicious gossip.
- Stealing from the victim.
- Extortion of money, food or homework.
- Physical violence, such as pushing, punching or pulling hair.
- Coercion.
- Isolation from groups.
Bullying is deliberately hurtful and difficult for victims to defend themselves against.
Children are the most likely group in the population to experience bullying, especially in a school environment, though it can take place in any setting, including home. If a foster parent (or member of staff) suspects or is aware that a child or young person is being bullied, the most important thing is to listen to the child or young person’s fears and worries, and then agree who should be told and what the child or young person would like to happen as a result.
Bullying at School
Schools are legally required to have an anti-bullying policy, and this should be made available to all pupils and their foster parents. The policy will outline the school’s procedure for responding to allegations of bullying. Foster parents should always request a copy when a foster child is enrolled. Foster parents and supervising social workers should always encourage and support young people who they believe are experiencing bullying at school to make full use of the school’s policy and procedures.
If foster parents think a fostered child is being bullied you should:
- Talk to the child about their experiences. Assure them things can be done to stop it.
- Keep a record of what the child says, especially of the incidents of bullying.
- Reassure the child that they are right to tell you about the bullying.
- Advise the child that they should report any further incidents at school to a teacher straight away.
- Discuss how to resolve the situation with your supervising social worker and the child’s social worker.
- Make an appointment to meet with the foster child’s teacher – explain the problem and agree on what the school will do to stop any further bullying.
- Keep a record of what has been agreed and make a time to meet the teacher again to discuss what progress has been made.
- If little progress has been made, discuss with your supervising social worker and the child’s social worker whether to request a meeting with the head teacher or register a formal complaint.
Foster parents must record all suspected or actual incidents and report these to the child or young person’s social worker as soon as possible.
Bullying in the Community
All suspected or actual incidents of bullying must be taken seriously and the incident fully investigated, either by the responsible local authority or Fosterplus, with support provided to the child or young person as well as their foster parents.
The foster parent and social worker should formulate a plan to address the concerns and this should include:
- Who should talk to the child or young person?
- Who else needs to be notified (e.g. schools, birth parents).
- Whether any immediate action is needed to safeguard the child/young person.
The plan should involve any relevant others, including:
- The foster child or young person.
- Other children or young people in the household.
- The foster child’s birth parents.
- The bully.
- The social workers and parents of other children in the foster home.
- Other relevant professionals such as teachers and therapists.
After the concerns have been discussed with the child or young person, if bullying is confirmed or continues to be suspected then a protection plan should be drawn up to attempt to ensure the bullying ceases and does not re-occur.
If the bullying is being done by someone outside the foster home, then attempts should be made to engage the bully’s parents or foster parents in helping to put an end to the bullying. The social worker for the child or young person, rather than the foster parent, should normally undertake any contact with parents or foster parents in such circumstances.
Bullying behaviours by a child
Foster parents who are concerned a foster child is bullying others should:
Bullying against foster parents
Foster parents who believe that they have been subjected to bullying by an employee of Fosterplus should follow the Complaints and Representations Procedure.
Cyber Bullying
Cyber bullying, also known as eBullying, is any form of bullying which takes place online or through smartphones and tablets – using social networking sites, messaging apps, gaming sites and chat rooms such as Facebook, XBox Live, Instagram, YouTube, Snapchat and other chat rooms.
Cyber bullying is meant to cause upset. It can be defined as simply as continuously sending an e-mail or messages to someone who does not want any further contact with the sender. It can also involve rude remarks (including gossip) about people over the internet via social networking sites like Facebook, Twitter, YouTube, WhatsApp, Tiktok, Instagram and Snapchat.
If children or young people have a mobile phone, you should advise them to be careful who they give the number to. Advise them that if they receive threatening or abusive phone calls, texts or e-mails they store the message (do not delete it) and tell their foster parent/s or someone else they trust. It is a criminal offence to send offensive or threatening phone messages, text messages or e-mails and, if it continues, it can also amount to harassment. The police can, and do, take action, but will need the messages as evidence.
Cyber bullying
The website https://www.kidscape.org.uk/cyberbullying/ has some very good advice for children and young people on protecting themselves from and responding to cyber bullying and covers:
- Abusive comments, rumours, gossip and threats made using digital communications and/or technologies – this includes internet trolling.
- Sharing pictures, videos or personal information without the consent of the owner and with the intent to cause harm or humiliation.
- Hacking into someone’s email, phone or online profiles to extract and share personal information, or to send hurtful content while posing as that person.
- Creating dedicated websites that intend to harm, make fun of someone or spread malicious rumours.
- Pressurising someone to do something they do not want to such as sending a sexually explicit image.
Internet Safety
All foster parents approved for placements of school age children should provide a personal computer suitably located within their home and available to foster children. The computer must have a Broadband connection to the Internet. Foster parents must take reasonable precautions to protect children from harm whilst they are using the Internet.
What risks do the Internet and Social Networking Sites present?
Foster parents need to protect young people, as far as possible, from the potential threats that some materials accessible online may present. The main dangers are from:
- Web sites on the Internet that contain pornographic, violent, racist or hate motivated material.
- Chat rooms or social networking sites that can provide opportunities for paedophiles to contact, and exploit young people. In addition, bullying, offensive and threatening language can feature.
- Unsolicited e-mail also known as Spam. Once it was dominated by pornography, but now it is often used for advertising and scams and may carry malicious software.
- Viruses or Worms that are often distributed by email as an attachment, or by a website containing malicious software. These are programs that install themselves into your computer software, causing malfunction and damage. Some malicious software can transfer all the information stored on the computer to another source unbeknown to the user.
- Phishing scams which are emails from companies or individuals that pose as someone such as your bank or possibly someone needing your help. They will try to obtain information such as passwords from you with the intention of stealing money or personal details. This can also lead to identity theft.
- Hacking – whilst connected to the Internet it is possible for someone to access your computer contents without your knowledge, if you do not have the correct firewall and antivirus products in place.
What do foster parents need to do to minimise risk?
- Install the computer in a room which will enable foster parents to monitor and supervise young people’s computer use; this is most likely to be the living room, (or the room where family members tend to spend most time).
- Educate young people about the potential dangers of the Internet, through discussion and use of written and on line materials.
- Use reputable Firewall and Anti-Viral protection programmes.
- Where a foster child has sole use of a computer or a foster child and their foster parent has shared use of the same computer, to install suitable security systems to reduce the risk of harm to the child.
- Draw up a Family Safety Code, so that everyone understands the rules for computer use.
Internet Safety eSafety Training
The Learning and Development Team commissions training for foster parents on Internet Safety eSafety – A guide for foster parents to safeguard young people’s use of the online world.
Please discuss with your supervising social worker how to access this course.
Example of a Basic Internet Family Safety Code
Acceptable use of the Internet
- No one is allowed to go to pornographic, racist, and violent or hate motivated web sites.
- No one must use abusive or threatening language in on line communication.
- Never download unknown files or illegal content (pirated music or movies) from the Internet.
- All family members under the age of 12 years should use a child friendly Search Engine – http://www.kidfriendlysearch.com/Kid_Friendly.htm
- All family members will keep all personal information secret: this includes, names, ages, addresses, landline and mobile phone numbers or personal financial details.
Providing details online
Sometimes, for registration purposes or buying on the Internet, some details may need to be provided. In all such instances:
- The responsible family member for providing such information is………. (foster parent).
- All family members will only use moderated and age appropriate chat rooms and social networks that have been agreed with by………. (foster parent).
- An online friend is a stranger in the real world and no family member should meet someone they have contacted on the Internet without the agreement of………. (foster parent).
- Any agreement will be given only on the understanding that …………. will be accompanied by………. (foster parent) and meetings must take place in a public place decided by ………… (foster parent).
- No family member should open unrecognised email or spam.
If things go wrong
- If any family member is upset by any communications received via the Internet, they should inform……….. (foster parent).
- If any family member is subject to inappropriate contact whilst using the Internet a complaint will be made to the Internet Service Provider. In the case of illegal materials or content the Police will be informed.
Computer security in the home
A number of technical options are available to foster parents to minimise the risks to young people. What are the right ones for an individual family will be influenced by the individual family member’s needs and the knowledge and competence of the foster parent in the use of computers.
Ensure you do not give administrative access to your computer to children. Administrator accounts on your computer give the user full access to all settings, which could enable the child to bypass any measures that you have put in place. Set up user accounts on your computer which only have limited access to the computer’s settings. Use different passwords for each account.
Foster parents who feel they have limited knowledge or skills are advised to provide Internet access through a Search Engine designed for children. This will help to filter out inappropriate content. There are several options, including one provided by Google – http://www.kidzsearch.com/. This is also the safest option for all children under the age of 12 years.
Foster parents will need to take a close interest in what the family computer is being used for and by whom. Regular monitoring and supervision are essential to ensure young people can achieve, learn from and enjoy the online world. By providing this range of technical equipment and safety measures, young people can enjoy and make positive use of the Internet. However, if foster parents have concerns that a young person is not using the computer for the purposes for which it is provided, they should always discuss with their supervising social worker and agree any appropriate actions or sanctions.
Age classification: films, games and online content
Introduction
In order to protect children from unsuitable or potentially harmful content in films, DVDs and some online entertainment services, the BBFC (British Board of Film Classification) provides a system of classification to give consumers information about the suitability of the content for children of different ages. Shops must not sell DVDs to children who are younger than the age stated, and cinemas must not admit children to view a film if they are underage. The BBFC considers issues of discrimination, drugs, language, nudity, sex, dangerous and imitable behaviour, and violence.
PEGI (Pan European Game Information) provides a similar service in relation to video games. Shops must not sell games to children who are underage.
BBFC ratings for film, DVD and online content
- U (Universal, suitable for all ages)
- PG (Parental Guidance – general viewing). Might be unsuitable for very young children, but should not unsettle a child aged 8 years or older
- 12A/12 (suitable for children aged 12 years and older). 12A is used for cinema release and 12 for DVD. A child aged under 12 years will be admitted to a cinema showing of the film if they are accompanied by an adult
- 15 (suitable for 15 years and older)
- 18 (suitable for 18 years and older)
PEGI game ratings
- 3 (considered suitable for all ages)
- 7 (generally suitable for all, but might contain fighting scenes)
- 12 (games that involve slightly graphic violence towards fantasy characters, or non-graphic violence towards human-looking characters/recognisable animals. Might involve some non-graphic nudity and mild swearing)
- 16 (depiction of violence or sexual activity is realistic, more extreme bad language, depiction of drugs criminal activity)
- 18 (depiction of gross violence that could cause a viewer to feel revulsion)
Using the classification system in your home
You should not purchase DVDs or games for children if they are underage, and you should not permit them to watch films or play games that are not considered suitable for their age at other locations (e.g. school, friends’ houses).
Making judgements about the suitability of a PG-rated film, or a 12A cinema release involves a careful consideration of the content and the likelihood that the young person might be unsettled by viewing it. A parent is entitled to make this judgement and it therefore falls within the remit of delegated authority, and should be discussed at the placement planning meeting and/or Care Plan review meetings. If you are not sure that you have been given delegated authority to make this decision, please discuss the issue with the young person’s local authority social worker.
Parental control software of mobile devices permits you to restrict online content in accordance with BBFC guidelines. Discuss this with the local authority for each young person and agree appropriate restrictions. These restrictions should be included within the young person’s risk assessment and safer care plan.
Staying safe online
The Child Exploitation and Online Protection (CEOP) Centre is the UK’s national law enforcement agency that focuses on tackling the sexual abuse of children. It has a thinkuknow website where you can find the latest information on websites, mobiles and new technology resources for those who work with children and a place to report any concerns about someone a child may be chatting to online. The site contains good information and safety tips: www.thinkuknow.co.uk
Further information on staying safe on line can be obtained from:
Social networking sites – foster parents
Social networking sites are widely used by foster parents and children as a way of keeping in touch with family and friends. However please do not upload photographs of children in your care on your Facebook page or other networking sites, for example Instagram or Twitter. There are some potential dangers, due primarily to the fact that accounts can be easily accessed unless appropriate levels of security are set by the account holder. Foster parents must use the Privacy Settings to limit access to their account to people they trust. Foster parents who feel there are positive reasons for a former or current foster child as an on-line friend should first discuss this with their supervising social worker and obtain their agreement.
But remember, Privacy Settings do not guarantee 100% security. Foster parents are strongly advised not to make any reference to a fostered child whilst using a social network site as this may breach their right to privacy. Foster parents should not communicate any work related information that is of a confidential nature on a social network site including any information that may identify a foster child. For example, some birth parents who are legally prevented from having contact with their children may try to use sites to trace their whereabouts or use personal information logged by a foster parent to discredit them.
Social networking sites – children
A majority of children use social network sites. Such sites are therefore an important way in which young people choose to stay in touch and communicate with friends. However, there are potential dangers; for example, from predatory adults pretending to be a ‘friend’, in order to gain access to vulnerable young people. Foster parents should take the risk minimisation steps identified above.
The younger the child the more closely the foster parent should oversee the child’s activities. If young people want to upload photos of themselves, encourage them to use pictures you both agree are suitable. Advise young people against entering details such as their phone number or address or any information that can identify their whereabouts. The foster parent should ensure that, should they become aware of any inappropriate photos of a child placed with them being put on social networking sites, they do not download them and forward/distribute them to other professionals involved with the child. It is illegal to distribute inappropriate images of children, whatever your motivation. Bring their presence online to the attention of the professionals.
Educate young people about cyber bullying and encourage them to tell someone they trust if they are subjected to bullying. The Child Exploitation & Online Protection (CEOP) Centre is the UK’s national law enforcement agency that focuses on tackling the sexual abuse of children and provides advice on steps that adults and young people can take to keep themselves safe. www.thinkuknow.co.uk.
Responding to Sexting (Youth Produced Sexual Imagery)
What is ‘Sexting’?
Youth Produced Sexual Imagery (“sexting”) can be defined as images of videos generated by children and young people that are of a sexual nature or are considered to be indecent. These images may be shared between children and young people and/or adults via a mobile phone, webcam, handheld device or website/app.
Sexting & sharing of naked images
There is an increasing trend for young people to take photographs of their breasts and genitalia and share this by mobile phone or social media with their boyfriend/girlfriends. Some young people are also exposing themselves on webcam both to the people they know and strangers within chat rooms. It is vital that young people know that when they send such images, they lose control of them and could find that they are shared beyond the recipient. The images can be taken and placed anywhere online without their permission. There is an additional risk that eh recipient will use the image in future to blackmail the young person.
Young people also need to know that creating and distributing these images can be a crime, if the young person pictured is under 16. Being convicted of distributing “indecent images” of children could result in a prison sentence (for those aged 16+) or admission to secure accommodation. It will also go onto affect the young person’s career and travel opportunities. The message to young people is clear:
- Do not take indecent images of yourself
- If you receive an indecent image, delete it without saving or sharing it.
It is important that young people know that if anyone is making them feel uncomfortable online and asking them to take indecent images of themselves that they can:
- Tell you
- Report the other person to CEOP, particularly if the required comes from someone they don’t know. You can make a CEOP report at www.thinkuknow.co.uk
- Use helpful apps such as Zipit, which was created by NSPCC to respond to request from boyfriends/girlfriends in a humorous way.
The law and youth produced sexual imagery
It is an offence to “communicate indecently” which includes the sharing of images via text, electronically (social media) or verbally, with any person who did not consent to receiving the communication, or that the person sharing this knows that the recipient does not consent. (Sexual Offences (Scotland) Act 2009).
The Act maintains the age of consent at 16 and provides that any sexual activity between an adult and a child or young person constitutes a criminal offence. Sexual intercourse and oral sex between children and young people under the age of 16 is unlawful.
Definitions
- “Indecent” can include images or verbal descriptions of penetrative and non-penetrative sexual activity
- “Making” can include opening an attachment, downloading images and saving images to a computer/mobile device online
- “Sharing” includes sending by email, offering on a file sharing platform, uploading to a site that other people have access to, and possessing with a view to distribute or a sexually explicit conversation.
Examples of offences:
- A young person under 16 years of age taking a nude photograph of themselves, possessing the image and sending it to another person.
- A young person under 16 years of age who receives a sexual image of another young person aged under 16 years, and keeps this image on their phone
- A young person under 16 years of age who receives a sexual image of another young person aged under 16 years, and forwards the image to a friend
- A person over the age of 16 who creates/possesses and/or shares a sexual image of a young person under the age of 16 years
If an incident of ‘sexting’ involving children under 16 is reported to the police, their initial response will be to discuss with social work colleagues and agree whether the offence is considered solely a criminal office or merits a joint investigation by Police and Child Protection Social Workers.
For young people aged 16 + who are subject to a supervision requirement Police Scotland may decide to adopt a similar process to that outlined for children under 16 above. However this will depend upon the circumstances of the sexting incident.
In deciding this the police may consider whether;
- The alleged activity has been shared with a number of recipients
- The alleged activity has been shared with an intent to cause harm or distress
- The alleged activity was solicited by an adult or an unknown person online
- The alleged activity was solicited by threats or deception
Young people’s devices might be seized by the police as evidence, although this action is avoided wherever possible as typically the device cannot be returned due to the technical difficulties in completely removing images from electronic devices so that they are irretrievable.
The subsequent investigation will consider whether the incident involved consensual sharing of images between individuals of a similar age, or adult where there could have been and evidence or coercion/violence/threat/profit making/revenge. Where offenders/victims are looked after children, child protection procedures are usually initiated.
Irrespective of the nature of the offences, and the circumstances involved, a referral to the Children’s Reporter is likely to be made, to enable the offences to be considered by a Children’s Hearing (for children under 16). The hearing will consider the support plans developed by social work for the young people involved to prevent recurrence of the incident.
Agency response
Foster parents should report any known/suspected incidents of youth produced sexual imagery as a notifiable event. Foster parents should notify their allocated SSW of the incident as soon as they become aware, or involve the out-of-hours service if the situation is outwith normal office hours. The agency will inform the Local Authority of the situation and the local authority will discuss the situation with their JIIT (Joint Investigative Interviewing Team) or equivalent. The JIIT is a combined police/social work team whose primary focus is child protection and investigation.
The Agency will also provide a notification to the Care Inspectorate.
The young person’s risk assessment will need to be updated, and a CSE risk assessment might be undertaken.
Support will need to be offered to the young person throughout the investigation, to include emotional support regarding the impact of the incident on their wellbeing and information about the JIIT investigation and any consequences thereof. This might include therapeutic support.
N.B. Agency staff and foster parents must not print, forward, distribute or save any youth produced sexual imagery unless instructed to do so by the police.
Access to television, videos and adult magazines
Through a number of media – including terrestrial television, cable or satellite TV, the Internet, videos, DVDs and magazines – it is possible to access a range of sexually explicit, obscene, violent and racist materials. Foster parents , along with others responsible for the day to day care of fostered children, have a duty to ensure that children in their charge are protected from these images.
Fosterplus expects that foster parents will make responsible decisions about the suitability of videos and DVDs, bearing in mind the censors’ classifications of a film. Similarly, foster parents must ensure that children and young people are unable to access unsuitable, adult oriented cable and satellite television channels. These are generally, subscription channels. It is possible to exclude access to such channels, and foster parents should contact their supplier for advice, if necessary.
Photography and videos
There are no routine restrictions on foster parents taking family pictures of their fostered child, or of the child and their friends. Foster parents do not need consent for this. But permission is required if they are to be used publicly for example the Fosterplus newsletters or school newsletters. Placement plans should also confirm that foster parents can give consent for formal school photographs. These should be encouraged to ensure children have school and group photographs taken as part of their life history. It is important that fostered children have a record and memories of their childhood and photographs can be a helpful way for fostered children to make sense of their history and can contribute to their life story book.
However, decisions on whether foster parents can consent to other types of photographs or media activity can be more problematic, where issues of confidentiality and safeguarding can be present. We also have to factor in the age and competency of a young person to make informed decisions. It should be assumed that many young people aged over 16 will very much take the ‘lead’ in these decisions.
Many children and young people take part in activities, in school, leisure, social or sporting settings, that may lead to publicity in the media. Others wish to engage in paid or voluntary activities which drive improvements in foster care and that may attract media attention. While this should be normally encouraged and celebrated, the issue of ‘who consents’ needs to be carefully judged in relation to particular known risks to the safety of an individual child.
Young people and foster parents often feel they are struggling with blanket policies in these areas, so individual consideration of each case is important. Any restrictions on a child’s photograph or name appearing in the media should be based on good explanations and clearly specified in the placement plan. If foster parents anticipate that these sorts of issues may arise, they need to bring them to the attention of their supervising social worker as early as possible.
Support Network
There may be occasions when foster parents need to have a break from the child they are caring for; this may be for personal or family reasons or to take a short holiday.
Where these are occasional or infrequent absences by the foster parent, it may cause the least disruption to a foster child if relatives or friends of the foster parent (who are known to the foster child) act as ‘temporary’ foster parents. Such ‘temporary’ foster parents are known as the support network. They will need to be assessed and checked by a supervising social worker.
In addition to assessing your support network, Fosterplus also recognises the importance of ensuring that any support network have been sufficiently prepared for the task and understand the regulatory framework within which they will be accountable, as well as where advice and support can be accessed.
Adults planning to stay with foster parents
The foster parent agreement requires any foster parent to give reasonable notice to Fosterplus of any plans to allow another adult to stay at their own home. Foster parents who neglect to do this would be in breach of the foster parent agreement and it may result on them being taken back to the Fostering Panel for a review.
We require that Disclosure Scotland checks are taken up on any person, over the age of 16 years, who wishes to join the household of a current foster parent. If it is a short holiday, attending a family event such as a wedding or simply a social visit, in such circumstances, the foster parent must not leave any fostered child in the sole care of the adult overnight.
Because of the legal status of fostered children, Fosterplus has a duty to ensure that any adult who plans to stay at a foster parent’s home is subject to an appropriate level of scrutiny, to establish that they are ‘safe’ and ‘suitable’. If we are unable to establish this or conclude that the adult is unsafe or unsuitable, we will refuse such a proposal.
The most likely reasons an adult plans to stay at the home of a foster parent are:
- They are the new partner of an existing foster parent.
- They are to look after the foster children, in the absence of the foster parent, as a short term arrangement (including where the foster children stay at the home of the temporary foster parent).
- For a short visit for such reasons as holidays, family events e.g. birthdays, Christmas celebrations, social visits.
- There is a change in the adult’s personal circumstances; such as ill health, marital breakdown, financial loss etc. As a consequence, the adult may not be able to continue to maintain their pre-existing living arrangements or accommodation. The main reason for the proposed move to the home of the foster parent is other than for direct involvement in the fostering activities of the foster parent.
Significant Relationship Policy
Fosterplus will only consider adults joining fostering households who are relatives or close friends. This excludes such people as lodgers (including foreign students), due to the difficulty in undertaking a meaningful assessment and vetting process and the likely temporary nature of such arrangements. In the event of a new partner who is having contact with foster children or intends to move into the house, Fosterplus will follow the significant relationship policy.
This is required when a foster parent forms a new relationship which brings the person into contact with foster children. It has a staged response depending on the level of involvement.
This policy can be downloaded from CHARMS/Download.
Holiday with friends and relatives of foster parents
There is no requirement that where a looked after child visits or spends a holiday with their foster parent’s friends or relative that the individual must be approved as a local authority foster parent, as the child will remain formally placed with their usual foster parents. There is also no statutory duty for Disclosure Scotland disclosures to be sought in relation to adults in a private household where a child may stay overnight or visit.
Ideally, such arrangements will be planned, authority agreed in the placement plan or at a LAAC review. Where this has not occurred, we would expect foster parents to raise the prospect of a holiday or school trip, sufficiently ahead of time, with their supervising social worker.
Holiday Planning Guidance
Introduction
Where possible, Fosterplus will support and encourage foster parents to take foster children on holiday either within the UK or abroad. For children who are fostered there needs to be a clear process and plan developed to ensure the safety of all who are participating in the holiday.
Foster parent’s Holiday Homes
Many foster parents have holiday homes that will have been assessed as second homes and a H&S risk assessment undertake on these properties by the SSW. This needs to be updated alongside the home H&S assessment as part of the review cycle. A holiday risk assessment in respect of the children currently in placement requires to be completed and shared with the LASW prior to going to the holiday home. This does not need to be completed each time you go to the holiday home except if there is a change in placement or different foster family members visiting and staying over in the holiday home.
Please note that if the holiday home is in another country including England, Wales or Northern Ireland, then the LASW should be advised as soon as possible so that any legal notifications e.g. Children’s Reporter, can be made. This is particularly important if the child in your care is placed on a named place of residence.
All other holidays including travelling abroad
We recognise that at times there are holiday special offers that may require the holiday to be booked prior to the points below being completed, however you should only do this if you have had a discussion with your SSW or another member of the Fosterplus team who have then had a discussion with the child’s social worker and their agreement has been given to book the holiday.
In giving agreement your SSW or the LASW will provide guidance in relation to sleeping arrangements/bedroom sharing, permission to travel abroad, and insurance cover required prior to booking a holiday.
- Discuss your intention to plan a holiday with your SSW as soon as possible and, where you are planning to use an hotel, or go abroad, prior to confirming any booking with a holiday company. This allows us to have discussions with the placing social worker for the child placed and ensure that the plan will not impact upon the care plan arrangements for the foster child, and enable appropriate checks and documentation (for example passports, parental consent) to be progressed prior to the holiday.
- A holiday risk assessment form has been developed for use to collate the core information to help you, the placing social worker and the agency have clear understanding of the location of the holiday, the sleeping arrangements, and the plans should there be a need for Fosterplus or the Local Authority to respond to an emergency whilst you are on holiday.
- The form needs to be completed by your SSW alongside yourself and shared with the LASW so that they can seek agreement from their council in relation to the plans being made.
- A completed copy of the form will be uploaded to the child’s Charms record, and a copy will be sent to the LASW for their records.
- Fosterplus OOH system will be advised that the holiday is taking place and the LASW will update their own OOH system.
Overnight stays and visits
General principles
Guidance on Overnight Stays
There is no legal requirement to undertake disclosure checks on adults in a private household where a looked after child may stay overnight. Disclosure checks should not be sought as a precondition of an overnight stay unless There is evidence to suggest that this may be necessary. If a foster parent has serious worries about an overnight stay invitation then it should be refused. If permission for an overnight stay has been refused, this should be based on clear, recorded reasons that are necessary to protect the child’s welfare in his or her particular circumstances. The child’s views should also be recorded. As far as possible the reasons should be shared with the child or young person, although care needs to be taken not to disclose confidential information about a third party.
Children need to feel able to stay with their friends and Fosterplus does not wish to impede this, but nonetheless Fosterplus and foster parents have a shared responsibility to ensure the safety of children in their care. Parents routinely make judgements on whether or not there are known risks to staying in a particular household or visiting relatives, and similar judgements should normally be made for children in foster care by their responsible foster parents. Judgements should be based on a reasonable assessment of risks, which at times will require consultation with your supervising social worker and/or the child’s social worker.
In all cases, we will seek to ensure that foster parents are fully aware of any specific individuals, addresses or areas which may place a child at risk and this information should also be included in the child’s placement plan. At the placement planning stage and all subsequent LAAC reviews, it is essential that foster parents and supervising social workers establish clearly what decision making powers are delegated to the foster parent in responding to a child’s request to stay overnight and/or visit with a friend.
Checklist for decisions
The following factors about the looked after child should be considered when making a decision about an overnight stay:
- The views of the child or young person on their friend and his/her family.
- If the child were subject to a supervision requirement specifying where the child is to reside, would an overnight stay conflict with any other terms of the supervision requirement or with the expectations of the children’s hearing? If so, the overnight stay cannot take place. Was the possibility of overnight stays discussed at the most recent hearing? If not, then the issue should be raised at the next hearing.
- The child’s age and level of maturity. Is the request appropriate to their age and are overnight stays common among children of their age?
- Has the child or young person stayed overnight with a friend before? If so how did they cope and did they enjoy the experience? Is there any evidence that they said they were staying at one friend’s house but moved on to another house without letting their foster parent know? If they have not previously had an overnight stay, are they ready now?
- Is the overnight stay likely to cause conflict with other aspects of the child’s life for example, the need to finish a project for school or visit their family? Can ways be found to fit in both activities?
- Is the child’s legal status one where their parents’ permission for an overnight stay should be taken into consideration?
- Does the child or young person have any health problems or disabilities that may affect the overnight stay for example, wetting the bed, a need to take medication or the need for wheelchair access? The foster parent should discuss with the child or young person the information and advice needed to be shared with the family of the child’s friend (the ‘host family’) beforehand to make sure that the child has a safe and comfortable stay.
- Does the child or young person have any cultural or religious needs that may affect the overnight stay for example, a halal, kosher or vegetarian diet? The information and advice to be shared with the host family beforehand should be discussed with the child or young person, and how this will be done.
If in doubt about the appropriate decision or if there is reason to consider that a child or young person may be at specific risk in staying in a particular household, you should consult the Supervising social worker for advice.
Foster parents are still expected to inform their supervising social worker (in advance) of any overnight stays, in particular. We have a responsibility to know where the child will be sleeping and to ensure that the child’s local authority have an awareness of the arrangement. Should emergencies occur when foster parents have gone away, for example, the responsible adult/s can access our out of hours service and report any issues, seek advice etc. For this purpose, we must be clear on the child’s location.
What information do I need to obtain when a child stays away?
Foster parents should always have contact details for the household in which the child or young person will be staying. They should also make contact with the household beforehand, as would any good parent, to assist in assessing the request and to confirm arrangements and to ensure that the household where the child will be staying have, in turn, the contact details of the foster parent(s):
- Obtain an address and telephone number.
- Ascertain who will be responsible for the child.
- Personally speak to the responsible adult to satisfy yourself that they are suitable as a temporary foster parent and to check that the sleeping arrangements for the child are appropriate.
- Know when the child or young person is due to return home.
- Clarify what transport arrangements are needed to facilitate this.
Keep a written record of the steps taken to ensure the child will be safe whilst staying with a friend and of the actual dates agreed for an overnight stay.
Adult supervision of children
Children under 8 should never be left unsupervised in or out of doors. Children aged 8 to 16 should not be left on their own, unless agreed in the placement plan. Young people over 16 can be left alone, unless the placement plan states otherwise.
Risk assessments
An initial risk assessment is made during the matching process when a child is first referred to the placement team for a possible placement. This will determine whether there are any known risks that a child may present, either to themselves or to others. It is quite possible that a child will show behaviours that can be identified as risks, only after a placement has taken place. Fosterplus will request copies of any existing written risk assessments and initiate the completion of an updated Risk Assessment once the child is placed.
Family Safer Caring Plans
Fosterplus requires that each foster home produces a family safer caring plan. This enables families to record how they behave towards each other and what family rules are in place, especially in the area of safer caring. This document should be shared with fostered children prior to their placement, if possible, as it will help them understand the essential rules of the home, what is expected of them and what they can expect of you. This plan should be reviewed annually or whenever there is any change in the household membership.
Individual Safer Caring Plan
It is important for the foster parent to draw up a plan with the young person that is specific to their needs to ensure that everyone understands what is permissible and acceptable to both the individual young person and the foster parent.
Health and Wellbeing
Health & safety responsibilities
Fosterplus has designed a Foster Parent Health and Safety Handbook to assist prospective foster parents, assessors, approved foster parents and supervising social workers to plan and review home safety, including outdoor areas, second homes and vehicles.
Health checklist when children and young people are first placed
- Have you registered the child with your GP (if the child is not to remain with their own GP)?
- Have you checked with your supervising social worker or the child’s social worker that a health assessment (medical) has been requested?
- Have you made a dental appointment for the child?
- Does the child require an eye test?
- If caring for a baby, are you attending baby clinic for regular developmental monitoring?
- Is the child’s vaccination record up to date?
- Has any medication been prescribed by a GP or other health professional, are there arrangements for storing it safely and administering it in accordance with the prescribed dosage?
- Is there agreement from birth parents, those with parental responsibility or the responsible authority for administration of non-prescribed medication and first aid?
- Have you checked to see if the child is undergoing tests, checks or treatment that you need to keep up?
- Have you the necessary signed consent from birth parents, those with parental responsibility or the responsible authority before any planned treatment is commenced on the child?
Registration with the local GP
The child or young person in your care should be registered with your local GP as soon as possible after placement, unless continuing registration with the child’s current GP has been agreed in the placement plan or with the child’s social worker. Where possible, the child should be permanently registered with your GP, as otherwise their medical records are not requested and this limits the child’s access to secondary health care services.
Hot tubs
These are an increasingly popular addition to the home garden and holiday accommodation. They are, however, several potential risks including bacterial infection and drowning. If you have a hot tub at home, we will complete a health and safety risk assessment with you to ensure that children are safe.
Children and young people must not use a hot tub without an adult present, and they are not suitable for young children who cannot regulate their body temperature. There is no legal age restriction on the use of hot tubs, but RoSPA considers that hot tubs should not be used by children under 5 and for children over 5 this should be set at a lower temperature of around 35°C and a limited soaking time of 10 minutes is advised, as they are less able to regulate their body temperature. We will ask for the consent of children’s social workers before allowing them to use a hot tub.
Read RoSPA’s advice about hot tubs here. [https://www.rospa.com/leisure-water-safety/water/advice/hot-tub-safety]
When the hot tub is not in use, please cover it and lock the lid.
Regularly test the water quality in the hot tub, in accordance with the manufacturer’s instructions. Store cleaning chemicals in a secure place, where children cannot find them.
Hygiene is particularly important when it comes to hot tubs. Everyone should shower before entering the hot tub, and nobody should use it if they have an infectious illness or an open wound, however small, as this can lead to bacterial infection.
It is also important never to submerge your head in a hot tub as hair can be caught in the filtration system.
Evidence from research and practice shows that looked after children and
care leavers are more likely to experience health problems than young people in the general population.
Health assessments and planning for Looked After Children should be carried out within the Values and Principles of the Getting it right approach and applying the core components of the approach.
Guidance on Health Assessments for Looked After Children and Young People in Scotland
Frequency of health assessments
It is the responsibility of a local authority to ensure that health assessments are carried out for every looked after child. Therefore, it is the child’s social worker who initiates the process. Initial health assessments should be undertaken by a registered medical practitioner, while review health assessments may be carried out by an appropriately qualified registered nurse/midwife – for example, a school nurse, health visitor or member of a LAC Nurse Specialists team.
Comprehensive Health Assessment
Every looked after child or young person receives a comprehensive health assessment within four weeks of the NHS Board receiving notification (that an individual has become “looked after‟).
Guidance on Health Assessments for Looked After Children and Young People in Scotland:
In many situations, as for children and young people who are looked after, the Childs Plan will include contributions from different services and agencies including needs identified through specialist assessments such as the Health Assessment and the actions to address these needs. To ensure that a consistent approach is taken by services and agencies the GIRFEC National Practice Model, should be utilised as the framework for any assessment and planning.
Involving parents and those with parental responsibility
It is good practice to involve parents in health assessments to provide an opportunity to obtain child and family health history directly as well as to obtain consent to gather further necessary data from GPs, consultants and hospitals. Where a child is provided with accommodation by the responsible authority under section 25 the parents must be given the opportunity to be involved in the child’s health assessment and parental consent is required for a health assessment to proceed.
Health services for looked after children
Looked after children should have access to the full range of health services, including General Practitioner (GP), health visiting/school nurse, child and adolescent mental health, speech and language therapy, audiology, vision, health promotion, oral health, specialist, and sexual health services.
Guidance on Health Assessments for Looked After Children and Young People in Scotland
Comprehensive Health Assessments
Objectives of health assessment
The objectives of the health assessment are to:
- Provide an opportunity to collate and to analyse the child/young
- Person’s health history including antenatal, birth, neonatal, past
- medical and family history.
- To identify unrecognised/unmet health needs, ascertain if the
- child/young person has missed or has any outstanding appointments,
- and to plan appropriate action.
- To comprehensively assess the child/young person’s current physical,
- developmental and emotional health needs.
All assessments and planning by each Agency involved in a child’s plan should be constructed around the 8 wellbeing indicators; safe, healthy, achieving, nurtured, active, respected, responsible and included. The Child’s Plan should contain a holistic overview of all information gathered and assessments carried out and structured around the wellbeing indicators; a summary of how this information was considered in terms of the child’s circumstances identifying strengths and pressures; how specific actions/ priorities were identified; and detail of a clear action plan. This must include the health assessment and action plan. The comprehensive health assessment will lead to a single agency health plan that can be shared and integrated to develop the multiagency Child’s Plan. The initial health assessment should be submitted to the multi-agency plan in My World Assessment format – i.e. strengths and pressures around SHANARRI.
These should be reviewed at every LAAC review to ensure that health plans are being followed and any actions carried out.
Key health workers
All looked after children should have access to a LAAC nurse. The LAC nurse should co-ordinate children’s health care irrespective of the number of care placement moves, ensuring coordinated continuity of health care and avoiding repeated assessments.
Hospitalisation
If the child needs to go into hospital, foster parents must inform their supervising social worker and the child’s social worker. If this takes place out of office hours, foster parents must inform the out of hours worker. Admissions to hospital are matters that we must notify to the Care Inspectorate and it is vital that this is communicated immediately to the Agency.
Going into hospital is frightening and the child or young person is going to experience a further separation from people they know. In line with the principles of providing a secure base, foster parents should, if possible, stay with and remain available to them in hospital. Fosterplus may be able to provide assistance, if this means additional costs or the need for extra help.
Consent to medical treatment
Consent to medical or preventive treatment
In Scots law, when persons reach their 16th birthday, unless they lack the appropriate mental capacity, they gain the legal capacity to make decisions which have legal effect under the Age of Legal Capacity (Scotland) Act 1991.
However, even under the age of 16, a child can have the legal capacity to consent on his or her own behalf to any surgical, medical or dental treatment where in the opinion of a qualified medical practitioner attending the child, the child is capable of understanding the nature and possible consequences of the procedure or treatment (see section 2(4) of the 1991 Act).
- This is a matter of clinical judgement and will depend on several things, including:
- The age of the patient
- The maturity of the patient
- The complexity of the proposed intervention
- It’s likely outcome
- The risks associated with it.
- Consent for Health Professionals in NHS Scotland
If a child under the age of 16 is not capable of understanding the nature of the healthcare intervention and its consequences, then you should ask the child’s parent or guardian for their consent to proceed with the intervention. The Local Authority will require to authorise any health care intervention where permission is required. However in the case of emergencies where treatment cannot be delayed it will usually be acceptable for medical practitioners to provide medical treatment without obtaining consent where it is immediately necessary to save life or to avoid significant deterioration in the patient’s health. The treatment given must be no more than the immediate situation requires however.
Health promotion
Promoting the health of children and young people in foster care is very important if they are to grow into mature, stable, well balanced adults. Children often have poor health when they first become looked after, and fostering services have a duty to promote the health and development of children placed with foster parents. Attention must be paid to both their physical and emotional health. Foster care must provide a healthy environment, where children’s good health and wellbeing is promoted, their health needs are identified and services are provided to meet their needs.
Healthy eating
Healthy eating is all about making sure you get the recommended amounts of vitamins, minerals, proteins and carbohydrates as well as the right types of fats and sugars. Good healthy eating habits need to start early, but foster parents often have to deal with a child whose eating habits have developed in a deprived or unhappy atmosphere. Even where this is not the case, a child may refuse to eat unfamiliar food when they have just left home. All sorts of behaviours are possible; overeating, hoarding, stealing, being finicky, refusal, vomiting. Whatever the case may be, it is always best to avoid confrontation; find out what the child’s eating habits and preferences are and only introduce new eating experiences gradually, at the child’s own pace. This is especially important for children with disabilities who may need special diets or help with eating. Some of the approaches foster parents can take include: